Anatomy and Physiology
20 Vasculature

Na lā e lana ana ke koko.
The days when the blood circulates freely.
Youth.
‘Ōlelo No‘eau, compiled by Mary Kawena Pukui, #2247
Introduction

Figure 20.1: Formation of New Blood Vessels
![]() Chapter Learning Outcomes
Chapter Learning Outcomes
- Compare and contrast the anatomical structure of arteries, arterioles, capillaries, venules, and veins
- Accurately describe the forces that account for exchange
- List the major factors affecting blood flow, blood pressure, and resistance
- Describe how blood flow, blood pressure, and resistance interrelate
- Discuss how the neural and endocrine mechanisms maintain homeostasis within the blood vessels
- Describe the interaction of the cardiovascular system with other body systems
- Label the major blood vessels of the pulmonary and systemic circulations
- Identify and describe the hepatic portal system
In the previous chapter, we learn about the structure and the function of the heart. However, the heart doesn’t work alone. In this chapter, you will learn about the vessels that transport blood throughout the body and provide the physical site where gases, nutrients, and other substances are exchanged with body cells. When vessel functioning is reduced, blood-borne substances do not circulate effectively throughout the body. As a result, tissue injury occurs, metabolism is impaired, and the functions of every bodily system are threatened.
![]() Cultural Connection
Cultural Connection
Cultural Connection: Aʻa Lewalewa
Aʻa lewalewa, or aerial roots on the highly revered ʻōhiʻa trees, bear a strong resemblance to the small veins and arteries. In fact, the Hawaiian word aʻa means root, rootlet, vein, or artery.

Figure 20.2: Aʻa LewalewaʻŌhiʻa may send out aerial roots, known as aʻa lewalewa. Aʻa (root) lewalewa (dangling, hanging) likely develop in response to stress. Stress may come from the cracking of the tree’s bark (either from natural growth or injury), fire heat or smoke, insects, or disease.
20.1 Blood Vessel Anatomy
![]() 20.1 Learning Outcomes
20.1 Learning Outcomes
- Compare and contrast the three tunics that make up the walls of most blood vessels
- Distinguish between elastic arteries, muscular arteries, and arterioles based on structure, location, and function
- Describe the basic structure of a capillary bed, from the supplying metarteriole to the venule into which it drains
- Explain the structure and function of venous valves in the large veins of the extremities

Figure 20.3 Capillaries and the relationship between blood vessels
Similar to us traveling from one place to another through streets and highways, blood is transported through the body via blood vessels. Arteries are blood vessels that convey blood from the heart to capillaries, whereas s conduct blood from the capillaries back to the heart. Capillaries are the thin-walled vessels that exchange substances between the blood in the cardiovascular system and the surrounding tissues. In this way, blood vessels deliver nutrients throughout the body and remove waste products.
General Vessel structure
There are three layers to most blood vessel walls. These layers are referred to as tunics (coats) that surround the blood. The innermost tunic is called the . It is a single layer of squamous endothelium surrounded by a subendothelial layer of areolar connective tissue.
The middle layer is called the . This is a circular arrangement of smooth muscle cells with elastic fibers which allow for . Vasoconstriction narrows the , resulting in increased . When these cells relax it allows , dropping the blood pressure.
The is the outermost layer of blood vessel walls. It consists of areolar connective tissue with collagen and elastic fibers. These fibers anchor the vessel to surrounding organs. The tunica externa also contains the , smaller arteries feeding the thick wall of larger blood vessels.

Figure 20.4: Blood Vessels: shows the layers of the , vein, and capillary
Comparing Vessels
Arteries have a thicker tunica media and a narrower lumen compared to veins. Elastic and collagen fibers allow the walls to stretch and recoil. Due to their thick walls, these vessels are more resilient and resistant to changes in blood pressure.
Capillary walls consist of tunica intima. This is a single layer of endothelium and a basement membrane without a subendothelial layer. The thin walls allow for : rapid exchange of gas and nutrients.
Veins have a thicker tunica externa and a much larger lumen. These vessels have fewer elastic and collagen fibers. Due to the thin wall, the vessel collapses in the absence of blood. Many veins also contain valves to keep the ing in the correct direction.
Arteries
Elastic arteries
Elastic arteries are also known as conducting arteries. These vessels are nearest the heart and are responsible for conducting the blood from the heart to the smaller artery branches. These are the largest arteries (1-3 cm) and contain lots of elastic fibers. Every time the heart pumps blood, these vessels stretch to receive the blood. In between ventricular contractions, elastic arteries recoil delivering blood to muscular arteries. The major elastic arteries are the , , common carotid, and common iliac arteries.
Muscular (distributing arteries)
The muscular arteries have diameters ranging from 3 mm to 1 cm. As the name implies, these vessels have relatively more elastic fibers than other arteries. There are two layers of elastic sheets in walls: the internal and external elastic lamina. The internal lamina is between the tunica intima and media, whereas the external layer is between the tunica media and externa. Most named arteries are of the muscular type such as the brachial and coronary arteries.
Arterioles
s are the smallest arteries ranging from 10 μm to 3 mm. The larger arterioles have all three tunics. Smaller ones have only a thin endothelium and a single layer of smooth muscle cells. This smooth muscle is usually partially constricted, imparting a vasomotor tone. Arterioles are known as vessels due to their influence on overall blood pressure and the slow blood flow rate in downstream capillaries.

Figure 20.5 Types of Arteries and Arterioles Comparison of the walls of an , a muscular artery, and an arteriole is shown. In terms of scale, the diameter of an arteriole is measured in micrometers compared to millimeters for elastic and muscular arteries.
![]() Clinical Application
Clinical Application
Clinical Application: Atherosclerosis
Atherosclerosis is a progressive disease of elastic and muscular arteries. It is caused by the presence of atheroma, a plaque deposit on the luminal face of the tunica intima. This causes a narrowing of the lumen which increases pressure. Higher pressure speeds up plaque formation, further narrowing the lumen. This progression may lead to serious cardiovascular issues. Some of the risk factors include infection, trauma, hypertension, inflammation, hypercholesterolemia, and smoking. Potential treatments include angioplasty and bypass surgery. One complication of this condition is aneurysms, a ballooning outward of the artery due to plaque buildup. This ballooning increases the risk of rupture causing internal bleeding which can be deadly. The most common arteries at risk of aneurysm are the aorta and those at the base of the brain.

Figure 20.6: Atherosclerosis
Capillaries
Capillaries are the smallest vessels and connect arterioles to s. These tiny vessels are only 8 to 10 μm in diameter. Since red blood cells (RBCs) are about the same size, they must squeeze through in a stack-like formation called a rouleau. Capillaries are short too, averaging only 1mm. They consist of a simple squamous endothelium with a basement membrane. These are the exchange vessels that are responsible for delivering nutrients to, and removing wastes from, the tissues. The thin walls allow for rapid, efficient diffusion. Three types of capillaries serve different functions.

Figure 20.7: RBCs stacking in a capillary
Figure 20.8: Simple squamous epithelium with basement membrane
Continuous Capillaries
As the name implies, continuous capillaries have no breaks or spaces between cells: they continue from one cell to the next. Tight junctions connect adjacent cells but do not provide a complete seal. Intercellular clefts are small gaps between endothelial cells large enough to allow small molecules, such as glucose, to cross from the blood to the interstitial fluid (IF). Additionally, the thin squamous cells also allow very efficient gas exchange. These are the most common type of capillary in the body and serve most organs including muscles, skin, lungs, and the central nervous system (CNS).
Fenestrated Capillaries
Fenestrated capillaries are mostly continuous but do have pores (holes) called fenestrations. These are found in areas of the body where smaller proteins and molecules are needed to pass between the cardiovascular system and another organ. Fenestrated capillaries are common in the small intestine–the primary site of nutrient absorption–as well as in the kidneys where the openings optimize blood . They are also found in the choroid plexus of the brain and many endocrine structures, including the hypothalamus, pituitary, pineal, and thyroid glands.
Sinusoidal Capillaries
Sinusoid capillaries are also known as discontinuous capillaries. Here, there is an incomplete lining of squamous endothelial cells and the basement membrane also has gaps. Because of the large holes in these vessels, cells can even pass through. Sinusoid capillaries are found primarily in bone marrow and spleen. Recall, bone marrow is the site of hematopoiesis-generation of red blood cells, white blood cells, and platelets. Once formed, these cells and platelets pass through the large sinuses of sinusoid capillaries to enter the bloodstream. The spleen, on the other hand, is responsible for filtering out cells and large debris from the blood.

Figure 20.9 Types of Capillaries The three major types of capillaries: continuous, fenestrated, and sinusoid.
Capillary Beds
s are a group of capillaries that function together to provide nutrients to, and remove wastes from, the surrounding tissues. Capillary beds receive blood from a branch of arterioles, called s. Branching off of the metarteriole are capillaries, vessels that allow perfusion of the tissues. The metarteriole continues as a as it passes from the arteriole to the venous side of the bed. Separating each capillary from the metarteriole are . When relaxed, these sphincter muscles allow blood to pass into the capillaries allowing perfusion to occur. When constricted, blood bypasses capillaries, continuing through the metarteriole (thoroughfare channel). Either way, the postcapillary venules are the small veins receiving the blood from the capillary bed.
Precapillary sphincters control blood flow to organs depending on demand. Even at rest, these sphincters are constantly opening and closing with only about ¼ being open at any given time. This cycling is known as . Perfusion describes the flow of blood into capillaries. The precapillary sphincters determine the perfusion rate, the rate being significantly higher when open than when closed. Perfusion rate is expressed in terms of blood volume per unit time per weight of tissue being served (mL/min/g).

Figure 20.10 Capillary Bed In a capillary bed, arterioles give rise to metarterioles. Precapillary sphincters located at the junction of a metarteriole with a capillary regulate blood flow. A thoroughfare channel connects the metarteriole to a venule. An , which directly connects the arteriole with the venule, is shown at the bottom.
Venules and Veins
Venules are the smallest veins with diameters of about 8 to 100 μm. These vessels receive blood from thoroughfare channels and capillary beds. The smallest of these are comparable to capillaries themselves. The larger venules have all three tunics and are much larger. These vessels merge forming veins.
A vein is a blood vessel that conducts blood toward the heart. There are various sizes of veins. The small and medium veins are companion vessels with muscular arteries, whereas the larger veins are more comparable with elastic arteries. Larger veins tend to travel alongside elastic arteries. This helps disturb the blood to prevent pooling. Many veins have significant venous valves to prevent backflow, ensuring blood moves toward the heart. These valves are made of a thickened tunica intima with elastic and collagen fibers similar to the semilunar valves of the heart.

Figure 20.11 Comparison of Veins and Venules Many veins have valves to prevent backflow of blood, whereas venules do not. In terms of scale, the diameter of a venule is measured in micrometers compared to millimeters for veins.
Veins as a blood reservoir
While at rest, about 30 percent of the blood volume is in the pulmonary circulation and the heart chambers. Most of the blood is in the systemic circulation (about 70%). However, 55 percent of the total blood volume is in the veins and only 15 percent is distributed between the arteries and capillaries. In this way, veins act as a reservoir for the cardiovascular system. When a higher rate of oxygen delivery is needed, such as during exercise, venoconstriction (constriction of the veins) changes the distribution of blood putting more into arteries and capillaries.

Figure 20.12 Graphical View of Distribution of Blood Flow. Blood spends a higher proportion of time in systemic veins than in any other part of the cardiovascular system. This chart shows the hierarchical percentages of blood flow found within each circuit of blood flow (inner ring), within the arteries, capillaries, and veins of each circuit (middle ring), and within each specific type of systemic vessel (outer ring). (Image credit: “Distribution of Blood Flow” by Julie Jenks is licensed under CC BY 4.0) LibreText Ch 18
 |
 |
 |
Figure 20.13 Varicose Veins Varicose veins are commonly found in the lower extremities
![]() Clinical Application
Clinical Application
Varicose Veins
Edema may be accompanied by varicose veins, especially in the superficial veins of the legs. This disorder arises when defective valves allow blood to accumulate within the veins, causing them to distend, twist, and become visible on the surface of the integument. Varicose veins may occur in both sexes, but are more common in women and are often related to pregnancy. More than simple cosmetic blemishes, varicose veins are often painful and sometimes itchy or throbbing. Without treatment, they tend to grow worse over time. The use of support hose, as well as elevating the feet and legs whenever possible, may be helpful in alleviating this condition. Laser surgery and interventional radiologic procedures can reduce the size and severity of varicose veins. Severe cases may require conventional surgery to remove the damaged vessels. As there are typically redundant circulation patterns, that is, anastomoses, for the smaller and more superficial veins, removal does not typically impair the circulation. There is evidence that patients with varicose veins suffer a greater risk of developing a thrombus or clot.
| Arteries | Veins | |
|---|---|---|
| Direction of blood flow | Conducts blood away from the heart | Conducts blood toward the heart |
| General appearance | Rounded | Irregular, often collapsed |
| Pressure | High | Low |
| Wall thickness | Thick | Thin |
| Relative oxygen concentration | Higher in systemic arteries Lower in pulmonary arteries |
Lower in systemic veins Higher in pulmonary veins |
| Valves | Not present | Present most commonly in limbs and in veins inferior to the heart |
Table 20.1: Summary table of the differences between arteries and veins.
Circulatory Routes and Other Vascular Structures
The flow of blood does not always follow the artery-capillary-vein pathway. Anastomoses are blood vessels that bypass capillary beds altogether. Arterial anastomoses are where two or more arteries converge feeding the same area. Examples of arterial anastomoses are the superior and inferior epigastric arteries. Venous anastomoses occur when two or more veins join, such as the anastomosis of the basilic, brachial and s that drain the upper limb. Arteriovenous anastomoses allow blood to flow from an artery to a vein bypassing smaller arterioles and capillary beds. These shunts are common in the fingers, toes, palms, and ears and allow heat conservation during hypothermia.
A portal system is a blood pathway with two capillary beds in a row such as the hypothalamo-hypophyseal portal system between the hypothalamus and the anterior pituitary gland.

Figure 20.14: Illustration of the 3 types of anastomoses Anastomotic configurations depicted as enteric hand-sewn anastomoses. a End-to-end anastomosis between two segments of small bowel. b End-to-side anastomosis between two segments of small bowel. c Side-to-side anastomosis between small and large bowel
Illustration of artery-capillary bed-portal vein-capillary bed-vein
Cross-sectional area and blood flow

Figure 20.15: The different types of blood vessels. Types of vessels include Arteries, Elastic arteries, Distributing arteries, Arterioles, Capillaries (smallest blood vessels), Venules, Veins, Large collecting vessels, such as the , the jugular vein, the and the iliac vein. Venae cavae (the two largest veins, carry blood into the heart). Sinusoids – Extremely small vessels located within bone marrow, the spleen, and the liver.
| Type of blood vessels | Total cross-section area | Blood velocity in cm/s |
|---|---|---|
| Aorta | 3–5 cm2 | 40 cm/s |
| Capillaries | 4500–6000 cm2 | 0.03 cm/s[17] |
| Vena cavae inferior and superior | 14 cm2 | 15 cm/s |
Table 20.2: Blood Vessel relative cross-sectional area, and flow rate
Despite their small diameters, the total cross-sectional area of capillaries is much larger than both arteries and veins. This is because there are so many capillaries. Blood flow velocity is inversely proportional to the total cross-sectional area. Therefore, blood flows slowly through capillary beds which allows for more efficient perfusion of capillary beds and the surrounding tissues. Diffusion takes time. The slow flow allows nutrients and wastes to be exchanged between the capillaries and the organs they are serving.
Diffusion of substances
Oxygen, hormones, and nutrients move from blood to interstitial fluid by diffusing from areas of high concentration to low concentration. This concentration gradient also dictates the bulk flow of waste products, including carbon dioxide. The bulk flow route depends on particle size. Small solutes, such as molecular oxygen, can diffuse through endothelial cells or intercellular clefts. Larger solutes, such as smaller proteins, pass through fenestrations or gaps in sinusoids. Endothelial cells can take substances in by pinocytosis. An intracellular vesicle crosses a cell and secretes contents via exocytosis on the other side. This exchange on both the arterial and venous ends of capillary beds (both to and from blood). Some hormones and fatty acids are transported by this method.
Vascularization
A vascular tissue or organ means it contains blood vessels. Some organs are highly vascular. These are the metabolically active organs of the body such as the brain, skeletal muscles, and heart. Other organs do not need such a high amount of blood delivery. The structures considered to be avascular (not containing blood vessels) are tendons, ligaments, epithelia, cartilage, and the cornea and lens of the eye.
![]() Clinical Application
Clinical Application
Angiogenesis & Regression
is the growth of new blood vessels in response to other physiological changes. The increased oxygen demand accompanied by aerobic exercise induces angiogenesis of skeletal muscle organs. Gaining weight in the form of adipose tissue also increases vessel growth. A gradual blockage of some coronary vessels may also induce angiogenesis. Tumors are the result of unregulated fast-growing cells. Due to the high metabolic rate, these tissues need a large nutrient supply. Aggressive tumors are often associated with the ability to stimulate angiogenesis. The opposite of angiogenesis is regression. A sedentary lifestyle or weight loss may cause regression of some vessels.

Figure 20.16: Angiogenic switch and angiogenesis as a requirement for tumor growth
20.2 Hemodynamics
![]() 20.2 Learning Outcomes
20.2 Learning Outcomes
- Distinguish between systolic pressure, diastolic pressure, pulse pressure, and mean arterial pressure
- Describe the clinical measurement of and blood pressure
- Identify and discuss variables affecting arterial blood flow and blood pressure
- Describe blood flow in the venous system, how blood returns to the heart
- Discuss several factors affecting blood flow in the venous system
- Identify the primary mechanisms of capillary exchange
- Distinguish between capillary hydrostatic pressure and blood colloid osmotic pressure, explaining the contribution of each to net filtration pressure
- Compare filtration and reabsorption
- Explain the fate of fluid that is not reabsorbed from the tissues into the vascular capillaries
Blood Pressure
Perfusion, or blood flow, refers to how blood moves through a vessel, tissue, or organ. Blood flow is measured in terms of how much volume of blood moves through a structure per unit of time. For blood to flow through vessels of your body, it needs something to push and force it through the vessels. The heart is your body’s pump that drives perfusion and blood flow. The contraction of the ventricles of the heart generates blood pressure (BP), which is pressure inside your blood vessels that moves blood through the vessels in your body. This pressure is highest closest to the heart but eventually decreases as blood travels through smaller arteries and arterioles, even smaller capillaries, then the venules and veins of the venous system where the lowest blood pressures are found. This section focuses on hemodynamics, the forces, and factors that drive blood circulation, and direct how blood is circulated throughout your body.
Blood pressure not only moves blood through your blood vessels, but also pushes against the walls of the blood vessels and your heart, making blood pressure a form of hydrostatic pressure, covered elsewhere in this chapter (link to capillary exchange). All blood vessels–arteries, capillaries, and veins–have pressure. However, in clinical settings, blood pressure without any specific descriptors usually refers to systemic arterial blood pressure, or the pressure of blood flowing in your systemic arteries (as opposed to the pressure of blood in your pulmonary arteries). In clinical practice, systemic arterial blood pressure is measured in mmHg (millimeters mercury, a unit of pressure) and obtained using a (blood pressure cuff) over the of the arm.
Systolic and diastolic pressure
When healthcare professionals measure blood pressure, they record two numbers, for example, 120/80. These two numbers represent and , and systolic pressure is always the first of the two numbers.
Systolic pressure is the arterial pressure during systole of the left ventricle of the heart. When the ventricles contract, it increases the pressure within the ventricular chambers. This pressure pushes blood out of the ventricles and away from the heart. Diastolic pressure is the arterial pressure during diastole, the period of ventricular relaxation.
The blood pressure within your arteries fluctuates between systolic and diastolic pressures every time your heartbeats. As the cycle of contraction and relaxation increases and decreases the pressure of the ventricles, it causes corresponding changes in blood pressure in systemic vessels. These fluctuations in blood pressure dampen once arterial vessels narrow into arterioles and eventually capillaries (Figure 20.17).

Figure 20.17 Systemic Blood Pressure The graph shows the components of blood pressure throughout the blood vessels, including systolic, diastolic, mean arterial, and s. https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance#fig-ch21_02_01]
![]() Clinical Application
Clinical Application
High Blood Pressure
Blood pressure is important in moving blood through your vessels and throughout your body, but high blood pressure can also damage vessels in the heart and other organs throughout your body. Hypertension (HTN) is the medical term for abnormally high arterial blood pressure. According to 2017 American Heart Association guidelines, normal blood pressure is when a person has systolic pressure less than 120 mmHg and diastolic pressure less than 80 mmHg. If a person’s systolic blood pressure becomes greater than 130 or diastolic pressure becomes greater than 80, that person is considered to have hypertension. Different grades of hypertension become more dangerous as either pressure increases above normal. Hypotension, or abnormally low blood pressure, may also be a health concern. (Table 20.3: also see to AHA HTN guidelines: https://www.heart.org/-/media/Images/Health-Topics/High-Blood-Pressure/Rainbow-Chart/blood-pressure-readings-chart.jpg).
| Blood Pressure Category | Systolic mm Hg
(upper number) |
Diastolic mm Hg
(lower number) |
|
| Normal | Less than 120 | and | Less than 80 |
| Elevated | 120-129 | and | Less than 80 |
| High Blood Pressure
(Hypertension) Stage 1 |
130-139 | or | 80-89 |
| High Blood Pressure
(Hypertension) Stage 2 |
140 or higher | or | 90 or higher |
| Hypertensive Crisis
(Consult your doctor immediately!)
|
Higher than 180 | and/or | Higher than 120 |
Table 20.3 American Heart Association (AHA) guidelines for hypertension
Pulse pressure
As mentioned in the previous section, there is a difference between systolic and diastolic arterial pressures due to the contraction and relaxation of the heart. Pulse pressure measures the difference between systolic and diastolic pressures and can be represented by the following equation:
pulse pressure = systolic pressure — diastolic pressure
For example, a person with a blood pressure of 110/70 would have a pulse pressure of (110-70), which results in a pulse pressure of 40 mmHg.
Normal pulse pressure is generally at least 25 percent of the systolic pressure. A pulse pressure below this level is described as low or narrow. This may occur in patients with a low stroke volume, such as someone who lost a lot of blood following a traumatic car accident. In contrast, high or wide pulse pressure is common in healthy people following strenuous exercise. As their heart contracts harder, increasing its ventricular pressures and stroke volume, a person’s systolic pressure can increase dramatically compared to their diastolic pressure. For example, a person with a pulse pressure of 30–40 mmHg at rest may increase their pulse pressure to 100 mmHG. However, this pulse pressure should return to its normal resting pulse pressure after exercise. If pulse pressure remains high and stays at or above 100 mmHg at rest, it may indicate excessive resistance caused by a variety of disorders. Chronic high resting pulse pressures can damage the heart, brain, and kidneys, and warrant medical treatment.
Mean arterial pressure and perfusion
Notice that arterial blood pressure constantly fluctuates between systolic and diastolic pressure in Figure x.bp.spdp. In that figure, notice that there is a line that runs between the systolic and diastolic pressures. That line represents the , which is another way of measuring systemic blood pressure. MAP represents the “average” pressure of blood in the arteries at any given time and estimates the overall average pressure that moves blood into arterial vessels that perfuse and deliver blood to tissues. Direct measurement and calculations of MAP can be complicated to calculate directly, so MAP is approximated using either of the following equations:
MAP = diastolic BP + (systolic BP – diastolic BP) ÷ 3
MAP = ⅔ × diastolic BP + ⅓ × systolic BP
For example, in a patient with a blood pressure of 110/80, their MAP would be:
MAP = 80 + (110 − 80) ÷ 3 = 80 + 30 ÷ 3 = 80 + 10 = 90 mmHg
The normal range of MAP is between 70 to 110 mmHg and can be used as an indicator of overall blood flow and perfusion to tissues. If MAP falls below 60 mmHg for a long period, that could indicate that blood pressure may not be strong enough to perfuse and deliver blood to all tissues. A lack of blood flow to tissues could result in a condition called , or insufficient blood flow. Low blood flow can also result in a condition called , in which tissues are not receiving enough oxygen. Hypoxia is related but slightly different from the term hypoxemia, which more specifically refers to low levels of oxygen in arterial blood in systemic circulation. Neurons are especially sensitive to hypoxia and may die or be damaged if blood flow and oxygen supplies are not quickly restored.
Pulse
As the heart contracts and relaxes, the pressure within arteries also increases and decreases accordingly in response to the volume of blood ejected with each beat. The elastic fibers in the arteries help maintain these high pressures as they expand and recoil to accommodate the changes in pressure. This expansion and recoil, or your pulse, can be felt as a throbbing within certain arteries with your fingertips, or measured electronically.
Because a patient’s pulse is a result of their heart rate and function, it is measured as one of the essential vital signs at every clinical visit. Pulse is recorded as a numerical rate with units of beats per minute. Both the rate and the strength of the pulse are clinically important. A high or irregular pulse rate can be caused by physical activity or other temporary factors, but it may also indicate a heart condition if the patient has been at rest. The pulse strength indicates the strength of ventricular contraction and cardiac output. If the pulse is strong, then systolic pressure is high. If it is weak, systolic pressure has fallen, and medical intervention may be warranted. In a healthy patient, their pulse rate should match their heart rate, and a large difference may indicate a problem in circulation between the heart and where the pulse is being taken. Different pulse rates between the same artery on the left and right sides of the body may also indicate a circulatory problem on one of the sides of the body.
Pulse can be felt, or palpated, by gently placing the tips of your fingers across an artery located close to the body’s surface. Taking someone’s pulse only requires pressing lightly, you do not want to press forcefully because you will obliterate the pulse and close off the artery completely and not feel anything. The in the wrist or the in the neck are common sites for taking someone’s pulse, but any superficial artery that can be palpated can be used (FIGURE 20.18). Many electronic devices are also available to measure pulses, such as a pulse oximeter (which can measure both pulse and arterial oxygen content), or an electrocardiogram (which can provide a patient’s heart rate, which should match their pulse as mentioned above).

Figure 20.18 — Common pulse points https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance#fig-ch21_02_02
Blood pressure measurement
Blood pressure (BP) is one of the standard vital signs measured during almost every clinical visit. Current techniques of blood pressure measurement are based on a method invented by Dr. Nikolai Korotkoff in 1905, who was able to measure BP without the use of electronics or computers. Korotkoff’s method used a sphygmomanometer (blood pressure cuff), an inflatable cuff with a gauge that measures air pressure inside the cuff. The method requires the use of a stethoscope to listen to the sounds inside an artery while the pressure inside the BP cuff changes.
The general steps are broken down as follows:
- Locate the patient’s brachial artery by using your index and middle finger to feel for their pulse inside the crook of their elbow (antecubital fossa)
- Wrap an inflatable BP cuff snugly around the patient’s arm and align the cuff with the brachial artery at about the level of the heart
- Inflate the BP cuff until the gauge reads about 30 mmHg above the patient’s expected systolic pressure
- Place a stethoscope on the patient’s antecubital region
- Slowly release pressure from the cuff and listen for tapping or swooshing . When you first start hearing those sounds, record the number on the pressure gauge. That is your patient’s systolic pressure.
- Continue listening to the sounds, and when they disappear, record the number of the pressure gauge. That is your patient’s diastolic pressure.
Although there are five recognized Korotkoff sounds, only two are normally recorded. When you first inflate the cuff above the patient’s systolic pressure, that temporarily cuts off circulation to your patient’s arm because the cuff pressure is greater than the maximum systolic pressure inside their circulatory system. The lack of blood flow means no sound. However, when the cuff pressure dips below systolic pressure, then the blood vessel is partially open. This causes turbulence, in which small swirls and eddies disrupt the flow of blood through the vessel. This turbulence churns blood and causes sounds that can be detected by listening to a stethoscope. These sounds will continue until the cuff pressure drops below diastolic blood pressure. At that point, the pressure in the blood vessel will be greater than the cuff pressure regardless if the heart is in systole or diastole, and the internal arterial pressure will keep the vessel open. Blood in this open blood vessel will flow smoothly (laminar flow), which is why the turbulent sounds disappear once the cuff pressure dips below normal BP.
 |
 |
| Stethoscope | Sphygmomanometer |
FIGURE 20.19: Stethoscope, sphygmomanometer
https://wordpress.org/openverse/image/1c7f0f4c-4d6f-41b9-a6d1-49eda596f44d
https://wordpress.org/openverse/image/37e6a30e-ab5f-4ca0-b938-a212fa004dec
Stethoscope, sphygmomanometer. Steps to measure BP, labels on all equipment with a sidebar of karotkoff sounds
Hemodynamics: Blood Flow, Pressure, and Resistance
Cardiac output & blood flow
Cardiac output is the rate of blood flow from the heart from each ventricle and is measured in liters per minute. Anything that causes cardiac output to increase will also force more blood into vessels, thus increasing blood pressure and promoting blood flow. Accordingly, any factor that decreases cardiac output will decrease arterial pressure and blood flow.
Factors that increase cardiac output and blood flow include sympathetic stimulation (epinephrine and norepinephrine), thyroid hormones, and increased calcium ion levels. Factors that decrease cardiac output and blood flow include parasympathetic stimulation, elevated or decreased potassium ion levels, decreased calcium levels, anoxia, and acidosis.
The relationship between flow, pressure, and resistance
Blood flow may be represented as a variable F and summarized as F = P/R with P representing the pressure in the vessel and R representing resistance in the vessel. Resistance describes any factor that can slow or impede blood flow. This simple equation describes how if you increase the pressure in a blood vessel, you increase and speed up blood flow in the vessel. Conversely, if you increase the resistance in a vessel, you decrease and impede blood flow in the vessel. Vasodilation will decrease resistance and result in more blood flow, while vasoconstriction will increase resistance and impede blood flow.
Factors affecting resistance to blood flow
Blood Volume
The relationship between blood volume, pressure, and flow can be seen in the nature that surrounds us in Hawaiʻi. For example, consider the massive volume of water flowing from the Kolekole Stream as it rushes off the edge of ʻAkaka Falls. (Figure 20.20) Compare that amount of flow compared to the volume, pressure, and flow of water flowing from a gutter or drainpipe after a light storm. This comparison and relationship also extend to blood volume — as blood volume increases, both pressure and flow increase.
 |
 |
| Akaka Falls | Water trickling from a drain pipe |
Figure 20.20 — Picture of Akaka Falls compared with water trickling from a drain pipe
![]() Food and Environment
Food and Environment
What is Your Favorite Waterfall?
Each Hawaiian Island has amazing waterfalls. Maybe the most famous and best viewed Hawaiian waterfall in the world is Manawaiopuna Falls on Kauai, which is also known as Jurassic Falls for its use in several scenes from the 1993 film Jurassic Park. Because it is located on private land, this waterfall is not publicly accessible (unless you take a helicopter tour!). But, that’s okay. There are plenty of other beautiful waterfalls for us to enjoy! What’s your favorite?

Figure 20.21: Manowaiopuna (“Jurassic”) Falls. (from Wikimedia)
Your body tries to maintain homeostasis in your blood volume, so normally your blood volume changes very little. Low blood volume, or , may be caused by bleeding, dehydration, vomiting, severe burns, or diuretic medications that cause your kidneys to produce more urine. Hypovolemia is potentially dangerous because a decrease in volume also means a drop in blood pressure and flow, therefore, organs in your body may not receive enough blood. is a critical condition in which the heart cannot pump enough blood to perfuse the organs of the body due to a severe loss in blood volume and the corresponding drop in blood pressure and flow. Other regulatory mechanisms in the body will try to compensate and maintain blood pressure so that a person with hypovolemia may not show symptoms until 10–20 percent of their blood volume has been lost. In emergencies, intravenous fluid replacement or a blood transfusion may be used to increase the volume of fluid inside vessels and restore blood pressure, flow, and perfusion. Shock (also, ) is a general condition that includes hypovolemic shock and is a critical condition where the tissues of the body do not have sufficient perfusion and blood flow, which could result in damage or death to the tissues and organs of the person, or the person themselves.
, which is an excess of fluid volume, may be caused by water retention or increased blood osmolarity, such as that seen during hypernatremia (abnormally high blood sodium levels). Hypervolemia is often seen in patients with heart failure, liver cirrhosis, some forms of kidney disease, hyperaldosteronism, and some glucocorticoid treatments. Hypervolemia is often seen with in the same patient, due to the relationship between blood volume and pressure, and presents along with all the health complications of hypertension as mentioned in this chapter. Restoring homeostasis in these patients depends upon reversing the condition that triggered the hypervolemia and can be aided by reducing the amount of fluid in the body such as giving diuretics to remove fluids from the body.
Blood Viscosity
Viscosity is the thickness of fluids that affects their ability to flow. For example, water is less viscous than coconut milk. Coconut milk would be less viscous than poi. [Figure x.hemo.poi] The viscosity of blood is directly proportional to resistance and inversely proportional to flow; therefore, any condition that increases viscosity will also increase resistance and decrease flow. For example, imagine trying to use a straw to drink water, then imagine using the same type of straw to suck up poi through the straw. It will be much more difficult to suck up poi through the straw because there is more resistance from the more viscous poi. Conversely, any condition that causes viscosity to decrease (such as adding water to dilute the poi) will decrease resistance and increase flow.
![]() Food and Environment
Food and Environment
Poi
Poi is a traditional staple food in the Polynesian diet. The word, poi, originally denoted the action of pounding the food to a pulp and making it into a thick paste. In Samoa and other Pacific islands, poi is a thick paste of pounded bananas or pineapples mixed with coconut cream. In Hawaii, a corm of a taro plant is almost exclusively used to prepare poi. The peeled corms are cooked, pounded, mixed with water to the desired viscosity, and strained with a cloth to remove fibers. Traditionally steamed corms were mashed with a stone pounder on a heavy board hollowed on the top surface. There are two types of corms; soft and hard. The two different types should not be mixed because of their different consistencies. The flavor of poi is dependent on the preparation and variety of taro used. “Taro Varieties in Hawaii” book published in 1939 contains descriptions of 84 varieties of taro found in Hawaiʻi. By the way, despite it being commonly referred to as a “root”, a corm is not a root of a plant. It is a bulbo-tuber; a rounded underground storage organ that is a modified base of a stem.
[Reference: Bishop museum]
 |
 |
| Poi | Kuʻi Poi (pounding poi) |
Figure 20.22: Picture of poi and pounding poi
Blood viscosity does not normally change over short periods. The two primary factors affecting blood viscosity are formed elements and plasma proteins. Since the vast majority of formed elements are red blood cells (RBCs), any condition affecting erythropoiesis and the overall number of RBCs, such as polycythemia or anemia, can alter viscosity. Since most plasma proteins are produced by the liver, any condition affecting liver health and its functioning can also change the levels of proteins such as albumins and globulins, thus affecting viscosity and flow. Liver abnormalities such as hepatitis, cirrhosis, alcohol damage, and drug toxicities result in decreased levels of plasma proteins, which decrease blood viscosity. While leukocytes and platelets are normally a small component of the formed elements, there are some rare conditions in which severe overproduction can impact viscosity as well.
A common misconception is that anticoagulants such as heparin and warfarin affect viscosity. Anticoagulants are often called “blood-thinners” by clinicians, but that refers to their ability to prevent the formation of clots, not due to having effects on viscosity. Anticoagulants will help prevent blockages in blood flow by preventing the formation of a thrombus (clot) that could impede or block blood flow through vessels, but anticoagulants will not significantly affect the amount of formed elements or non-clotting factor proteins.
Vessel Length and Diameter
The length of a vessel is directly proportional to its resistance: the longer the vessel, the greater the resistance and the lower the flow. As with blood volume, this makes intuitive sense, since the increased surface area inside a longer vessel will have more friction that impedes the flow of blood. Likewise, if a vessel is shortened, the resistance will decrease and flow will increase.
The length of our blood vessels increases throughout childhood as we grow, of course, but is unchanging in adults under normal physiological circumstances. Further, the distribution of vessels is not the same in all tissues. Adipose tissue does not have an extensive vascular supply. One pound of adipose tissue contains approximately 320 km (200 miles) of vessels, whereas skeletal muscle contains more than twice that length. Overall, vessels decrease in length only during the loss of body mass or surgical removal. An individual weighing 70 kg (154 pounds) has approximately 97,000 km (60,000 miles) of vessels in the body. Gaining about five kg (11 pounds) adds from 3,200 to 6,400 km (2,000 to 4,000 miles) of vessels, depending upon the type of body mass gained. Weight reduction benefits the cardiovascular system by requiring fewer vessels and overall vessel length, thereby reducing vascular resistance and stress to the heart, which does not have to overcome the resistance of more numerous and lengthier vessels.
In contrast to length, the diameter (and radius, since diameter = 2 × radius) of blood vessels changes throughout the different types of vessels throughout the body, as discussed in the section comparing the types of vessels. The diameter of your blood vessels changes frequently throughout the day in response to neural and chemical signals that trigger vasodilation and vasoconstriction to maintain pressure, flow, and perfusion homeostasis. A blood vessel’s diameter is determined by the and contractile state of the smooth muscle in the tunica media in the wall of the blood vessel. Thus, the contraction of smooth muscle affects the resistance and flow through a blood vessel. The effect of vessel diameter on resistance is inverse: Given the same volume of blood, an increased diameter means there is less blood contacting the vessel wall, thus lower friction and lower resistance, subsequently increasing flow. A decreased diameter means more of the blood contacts the vessel wall, and resistance increases, subsequently decreasing flow.
The influence of lumen diameter on resistance is dramatic: A slight increase or decrease in diameter causes a huge decrease or increase in resistance. This is because resistance is inversely proportional to the radius of the blood vessel raised to the fourth power (R = (1/r)4). This means, for example, that if an artery or arteriole constricts to one-half of its original radius, the resistance to flow will increase 16 times. And if an artery or arteriole dilates to twice its initial radius, then resistance in the vessel will decrease to 1/16 of its original value and flow will increase 16 times.
generally refers to the ability of a blood vessel or any enclosed space to expand to accommodate an increase in its volume. A balloon would be considered compliant as it can expand with increased air inside its volume, but a glass bottle would not be considered compliant as it has a rigid structure and will not expand with increased contents.
If an artery is compliant, it will be able to expand and absorb surges in blood flow without increasing resistance or blood pressure. Veins are more compliant than arteries and can expand to hold more blood. Atherosclerosis is a hardening of the arteries that occurs when fats and cholesterol build up in artery walls, causing them to stiffen and lose compliance. This makes arteries less elastic and able to absorb changes in pressure, thus increasing the body’s overall blood pressure. Atherosclerosis also narrows the inside lumen radius of these vessels, causing increased resistance and reduced blood flow. The increased pressure and reduced blood flow force the heart to work harder to overcome these difficulties in blood flow. This is why diet is important in preventing atherosclerosis and maintaining a healthy cardiovascular system. Atherosclerosis is a specific type of arteriosclerosis. Arteriosclerosis is the general term for the thickening and hardening of arteries. Arteriosclerosis happens to people as they age but can also be caused by lifestyle factors such as diet and smoking.
Comparison of flow, pressure, and resistance across vessels
Recall that arterioles are also called resistance vessels because their small lumen diameter dramatically slows the flow of blood from arteries. Arterioles are the site of the greatest resistance in the entire vascular network. This may seem surprising, given that capillaries have a smaller size.
Figure 20.23 compares vessel diameter, total cross-sectional area, average blood pressure, and blood velocity through the systemic vessels. Notice in parts (a) and (b) that the total cross-sectional area of the body’s capillary beds is far greater than any other type of vessel. The total cross-sectional area is calculated by taking the diameter of a type of vessel and then multiplying it by the count of how many of those vessels there are in your body. Although the diameter of a single capillary is significantly smaller than the diameter of an arteriole, there are vastly more capillaries in the body than there are other types of blood vessels. Part (c) shows that blood pressure drops unevenly as blood travels from arteries to arterioles, capillaries, venules, and veins, and encounters greater resistance. However, the site of the most precipitous drop, and the site of greatest resistance, is the arterioles. This explains why vasodilation and vasoconstriction of arterioles play more significant roles in regulating blood pressure than do the vasodilation and vasoconstriction of other vessels.
Part (d) shows that the velocity (speed) of blood flow decreases dramatically as the blood moves from arteries to arterioles to capillaries. This slow flow rate allows more time for exchange processes to occur. As blood flows through the veins, the rate of velocity increases, as blood is returned to the heart.

Figure 20.23 Relationships among Vessels in the Systemic Circuit https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance#fig-ch21_02_04]
Venous return
You now know that blood pressure decreases as it circulates from the artery side of your systemic circulation to the venous side. You may be also wondering how your veins can maintain blood flow despite having a relatively low pressure compared to other blood vessels. But did you know that the heart is not the only pump that circulates blood in your body, and there are additional pumps in your body that help to circulate blood?
If blood is to flow from veins back into the heart, the pressure in the veins must be higher than the pressure in the atria of the heart. Two factors help maintain this pressure gradient between the veins and the heart. First, the pressure in the atria during atrial diastole is very low and almost zero when the atria are fully relaxed. Second, two physiologic “pumps” increase pressure within the vessels of the venous system, thus driving blood flow through veins.
Skeletal Muscle Pump
The refers to how in many body regions, the skeletal muscle that surrounds veins can contract and squeeze and increase the pressure inside those veins. A classic example of the skeletal muscle pump are the muscles in your calves and the veins found in that region (Figure 20.24). As the leg muscles (e.g., gastrocnemius and soleus) contract when you walk or run, they squeeze and exert pressure on nearby veins. These veins also have numerous one-way valves that point back toward your , which helps to maintain blood flow in the right direction. The combination of skeletal muscle contraction outside the veins and valves inside the veins helps to push blood back toward the heart. These forces help to counteract the effect of gravity, as gravity tries to pull your blood toward your legs when you are standing up. Military recruits are trained to flex their legs slightly while standing at attention for prolonged periods because failure to do so may allow blood to pool in the lower limbs rather than returning to the heart. Consequently, the brain will not receive enough oxygenated blood, and the individual may lose consciousness and faint. This is also why the calves are sometimes referred to as the “second heart” as they maintain a constant rhythm of pumping blood in your veins when you have a steady pace as you walk or run.

Figure 20.24: Skeletal Muscle Pump Contraction of skeletal muscles surrounding a vein compresses the blood and increases the pressure inside those veins. The one-way valves ensure that blood flows only in the proper direction and back toward the heart. https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance#fig-ch21_02_06 ]
![]() Clinical Application
Clinical Application
Varicose Veins and Hemorrhoids
Varicose veins are a condition of dilated and tortuous venous vessels caused by nonfunctional failed valves. The damaged valves allow blood to flow backward resulting in blood pooling, which causes the dilation of the vessels and ultimately causes damage to the vessel walls. Risk factors include genetics, age, excessive standing, obesity, and pregnancy. Hemorrhoids are a similar condition of damaged vessels in the anorectal region.
Respiratory Pump
The also aids blood flow through the veins of the thorax and abdomen. During inhalation, the volume of the thorax increases, largely through the contraction of the diaphragm, which moves downward and expands the lungs in that direction. The elevation and outward expansion of the rib cage caused by the contraction of the external intercostal muscles also contributes to the increased volume of the thorax during inhalation. The increased volume causes pressure within the thorax to decrease, allowing us to inhale. Additionally, as air pressure within the thorax drops, blood pressure in the thoracic veins also decreases, falling below the pressure in the abdominal veins. This causes blood to flow along its pressure gradient and move from the higher pressure in veins outside the thorax and into the thoracic region with its decreased pressure during inhalation. This also promotes the return of blood from the thoracic veins to the atria. During exhalation, air pressure increases within the thoracic cavity, and thus pressure in the thoracic veins increases. This increased pressure in the thoracic veins gives an additional push and speeds up blood flow into the heart, while valves in the veins prevent blood from flowing backward into the systemic circulation.
Venoconstriction in Resistance, Blood Pressure, and Flow
As previously discussed, vasoconstriction of a vessel decreases the radius, increasing resistance and pressure, but decreasing flow. Venoconstriction, on the other hand, has a very different outcome. The walls of veins are thin but irregular; thus, when the smooth muscle in those walls constricts, the lumen becomes more rounded. The more rounded the lumen, the less surface area the blood encounters, and thus the blood flows smoother with less friction and resistance. Vasoconstriction also increases pressure within a vein as it does in an artery, but in veins, the increased pressure increases flow. Thus, venoconstriction speeds up blood flow and increases the return of blood to the heart. This mechanism also works with preload [Link to heart chapter or glossary] in the heart, as filling the heart with more volume will increase the contraction of the heart, thereby increasing cardiac output and blood flow.
Venous Reserve
Even though the heart and arteries have the highest pressures and rates of blood flow in your body, and the capillaries are the most numerous types of vessels in your body; the venules and veins of your body contain about 64 percent of your body’s total blood volume (Figure: 20.25). Veins can store a lot of blood due to their large diameter, low pressure, relatively slow flow (Figure 20.25), and being highly compliant and flexible. This is also why veins are called vessels due to their capacity to hold large volumes of blood.
Approximately 21 percent of your total blood volume (about 1 L in a person with 5 L of blood) is contained within networks of veins in your skin, liver, and bone marrow. The collective volume within those tissues and organs is called the . Blood circulates through these tissues but flows relatively slowly under normal physiological conditions. However, in cases of hypovolemic shock or hemorrhage where a sudden drop in blood volume results in a drop in perfusion and blood supply to organs and tissues, the body can use venoconstriction to squeeze blood from the tissues that make up the venous reserve, thus adding volume back to other vessels leading to and from the heart and increasing the pressure and flow to those vital organs.
 |
 |
Figure: 20.25 Cardiovascular distribution of blood
Capillary exchange
Capillaries not only provide fresh oxygen and nutrients, but they also balance out the composition of fluids and molecules throughout your body. Capillaries also collect excess waste byproducts of cellular metabolism so they can be excreted out of your body. This is why capillaries are also called exchange vessels. Figure 20.23 shows that blood flow reaches its slowest pace as it travels through the capillaries that branch, perfuse, and nourish the tissues of your body. This slow rate of flow allows blood to spend more time in capillaries, thus allowing more time for exchange between the blood and surrounding tissues. Diffusion helps in the redistribution and exchange of molecules across a capillary, and the thin walls of a capillary help to shorten the distance a molecule needs to diffuse across the capillary walls. However, diffusion is not the only force driving capillary exchange. Diffusion is relatively small compared to other pressures that draw fluids in and out of capillaries.
Filtration and Reabsorption
Two major processes describe the overall movement of fluid into and out of capillaries. Filtration involves the forces that drive the movement of fluid from the inside of a capillary toward the tissues surrounding a capillary. Filtration is mostly due to the higher pressure inside a capillary bed compared to lower pressure in the interstitial fluid of the tissues surrounding a capillary. involves the forces that draw fluid from the tissues surrounding a capillary and bring those fluids back into the inner lumen of a capillary. Reabsorption largely involves soluble components and osmotic pressures that draw water toward regions of higher solute concentration.
Hydrostatic Pressure
Hydrostatic pressure is the primary force driving fluid out of capillaries and into tissues. More generally, hydrostatic pressure is defined as the pressure of any fluid within an enclosed space. is the specific force exerted by the blood contained within your cardiovascular system and presses towards the walls of your blood vessels and heart. Even more specifically, is the pressure exerted by blood against the wall of a capillary and is the same as capillary blood pressure. CHP is the force that drives fluid out of capillaries and into the tissues and is an average of about 35 mmHg on the arterial side of the capillary bed. However, as blood flows through a capillary bed, the capillary blood pressure and CHP also decrease toward the venous side. At the venous side of a capillary bed, CHP drops to about 18 mmHg.
As fluid exits a capillary and moves into tissues, the pressure of the interstitial fluid surrounding those tissues rises in turn. This opposing hydrostatic pressure is called the . The CHP originating from the arterial pathways is much greater than the IFHP because lymphatic vessels are continually absorbing excess fluid from the tissues and lowering IFHP to a minimal value close to 0 mmHg.
CHP and IFHP push fluids in opposite directions, but the CHP in capillaries far exceeds IFHP found in tissues, so hydrostatic pressure generally moves fluids from the inside of a capillary out toward the outside interstitial fluid.
Osmotic pressure
One way you can think about reabsorption is to break down the word into “absorption”, which means to take in or soak in something, and the “re-” prefix, which suggests that the process is happening again. In the capillaries, reabsorption allows capillaries to bring fluids back into its lumen and reclaim the fluids that were pushed out due to hydrostatic pressures.
Osmosis is the overall movement of water molecules across a semi-permeable membrane toward an area of higher solute concentration [see Osmosis section of Cell chapter]. Osmotic pressure is the force that moves fluids between two areas based on differences in solute concentration. Osmotic pressure is determined by osmotic concentration gradients, that is, the difference in the solute-to-water concentrations found in blood and interstitial fluid. Osmotic pressures will pull and draw water from regions that have lower solute concentrations and move it toward regions with a higher solute concentration.
Plasma and interstitial fluid have similar concentrations of electrolytes and ions such as Na+, Cl-, K+, and HCO3-. This is due to the small size of these ions and their ability to easily cross between the plasma and interstitial fluid at capillaries. However, larger molecules and cells cannot easily pass between the endothelial cells of a capillary. One important note is to recognize that the formed elements of blood do not contribute to osmotic concentration gradients. However, large plasma proteins, such as albumins, play a vital role in driving osmotic pressure at capillaries. These proteins draw water toward the charged amino acids and dipoles from polar bonds in their polypeptide structures, and the force specifically due to these proteins is called oncotic pressure. Blood plasma proteins have a large size and cannot filter out, thus oncotic pressure is largely one-sided and serves to draw water back into vessels and reclaim fluid volume.

Figure 20.26 Hydrostatic and Osmotic Pressure
As mentioned in the blood chapter, plasma is a colloid due to having large particles such as albumin evenly suspended in its volume, thus giving it a cloudy, opaque appearance. is the pressure created by the concentration of colloidal proteins, such as albumins in the blood, and exerts an average of about 25 mmHg of pressure that moves fluid back into capillaries, thus allowing capillaries to reabsorb water. The plasma proteins suspended in the blood cannot move across capillary cell membranes, and so they remain in the plasma. As a result, blood has a higher colloidal concentration than interstitial fluid. You can also think of colloid and albumins as allowing blood to retain and hold onto water. refers to the osmotic pressure of the interstitial fluid’s solutes and proteins, but since interstitial fluid contains few proteins and has similar ion and glucose concentrations to plasma, this pressure is nearly 0. Thus, BCOP is always higher than IFCOP and the movement of fluids is a lopsided balance that favors reabsorbing fluids back into the plasma found within capillaries. Therefore, BCOP is the main force that accounts for reabsorption.
Net filtration pressure
The previous sections establish that CHP is the primary force behind filtration at capillaries and driving fluid out from capillaries toward the interstitial fluid and that BCOP is the primary force behind reabsorption and bringing fluid back into capillaries from the interstitial fluid. It may seem unusual to think of osmosis as pressure in units of mmHg, but by using the same units of measurement, the two opposing forces can be compared and used to calculate and predict the overall movement of fluid between capillaries and the surrounding tissue.
describes and measures the overall balance between hydrostatic and osmotic pressures between a vessel and the surrounding interstitial fluid. Net filtration pressure is calculated by adding the forces that move and filter fluid out from a vessel and subtracting the forces that reabsorb fluid back into vessels (since filtration and absorption move in opposite directions). The net filtration pressure of a capillary can be calculated by the following equation:
NFP = CHP – BCOP + IFCOP – IFHP
NFP = net filtration pressure
CHP = capillary hydrostatic pressure
BCOP = blood colloidal osmotic pressure
IFCOP = interstitial fluid colloidal osmotic pressure
IFHP = interstitial fluid hydrostatic pressure
However, as mentioned in previous sections, IFCOP and IFHP are almost equal to 0 mmHg in most tissues, so the above equation can be simplified to:
NFP = CHP – BCOP
Given this equation, if CHP, and thus, filtration is greater than reabsorption due to BCOP, NFP will have a positive value. Therefore, if NFP is positive, fluid will filter out and have a net overall movement out of the blood vessel. NFP may be negative if BCOP and reabsorption are greater than hydrostatic pressure, which would result in overall reabsorption and movement of fluid back into capillaries.
Net filtration pressure is not constant throughout a normal capillary bed, as CHP decreases as blood flows from the arterial side of a capillary bed to the venous side. If we use the above NFP equation, we can calculate the NFP when blood first enters a capillary bed. The average CHP at the arterial side of a capillary bed is 35 mmHg, and the BCOP is 25 mmHg. Using the above NFP equation, we get:
NFP = 35 mmHg – 25 mmHg = +10 mmHg
Therefore, more fluid will filter out at the start of a capillary bed.
If we apply the same calculation to the venous side of a capillary bed, we will have a CHP = 18 mmHg (remember that blood pressure drops when traveling from arteries to veins) and BCOP = 25 mmHg (remember that blood proteins do not filter out, therefore, BCOP is constant). Using the above NFP equation, we get:
NFP = 18 mmHg – 25 mmHg = -7 mmHg
Therefore, NFP will be negative, and more fluid will be reabsorbed back into capillaries at the end of a capillary bed as it enters a venule. These forces are summed up in Figure 20.27.

Figure 20.27 Net filtration pressure along a capillary https://openstax.org/books/anatomy-and-physiology/pages/20-3-capillary-exchange#fig-ch21_03_01]
20.3 Lymphatic Structures
![]() 20.3 Learning Outcomes
20.3 Learning Outcomes
- Describe the structure and function of the lymphatic tissue (lymph fluid, vessels, ducts, and organs)
Lymph and fluid balance
Notice that the net filtration pressure between the arterial and venous ends of a capillary have different numerical values. Since the NFP at the arterial end is 10 mmHg going outwards from the capillary, and the NFP at the venous end is 7 mmHg going back into the capillary, there is more overall filtration than reabsorption at capillaries. This results in about 20 liters of plasma being filtered into the interstitial space of your tissues each day due to capillary filtration. Once this filtrate is out of the bloodstream and in the tissue spaces, it becomes interstitial fluid. Of this interstitial fluid, 17 liters are reabsorbed by the blood vessels. This imbalance means that there would be interstitial fluids accumulation in tissues if capillaries were the only vessels that affect fluid balance. When interstitial fluids accumulate in tissue, this is a condition called edema. How does your body maintain homeostasis in balancing fluids and manage the remaining three liters that would accumulate in your tissues? This is where the lymphatic system comes into play.
Vessels of the lymphatic system drain body fluids and return them to the bloodstream. Lymphatic vessels are found throughout almost all of the tissues of your body and drain excess fluid and empty it back into the bloodstream via a series of lymphatic capillaries, vessels, trunks, and ducts. Some organs and tissues do not have lymphatic vessels, including the central nervous system, bone marrow, bones, teeth, and the cornea of the eye.
Lymph is the term used to describe interstitial fluid once it has entered the lymphatic system. When the lymphatic system is damaged in some way, such as by being blocked by cancer cells or destroyed by injury, protein-rich interstitial fluid accumulates (sometimes “backs up” from the lymph vessels) in the tissue spaces. Lymphedema is the accumulation of fluid as a result of a blockage and may lead to serious medical consequences.
Lymphatic capillaries are formed by a one-cell-thick layer of endothelial cells and allow interstitial fluid to flow into them via overlapping cells (see Figure 20.28). When interstitial fluid pressure is low, the endothelial flaps close to prevent the “backflow” of lymph back into tissues. As interstitial pressure increases, the spaces between the cells open up, allowing the fluid to enter the lymphatic capillaries. Entry of fluid into lymphatic capillaries is also enabled by the collagen filaments that anchor the capillaries to surrounding structures. As interstitial pressure increases, the filaments pull on the endothelial cell flaps, opening up them even further to allow easy entry of fluid.
In the small intestine, lymphatic capillaries called lacteals are critical for the transport of dietary lipids and lipid-soluble vitamins to the bloodstream. The lipid-rich lymph becomes a milky fluid called chyle. The chyle then travels through the lymphatic system, eventually entering the bloodstream.

Figure 20.28: Lymphatic Capillaries https://openstax.org/books/anatomy-and-physiology/pages/21-1-anatomy-of-the-lymphatic-and-immune-systems#fig-ch22_01_02
Lymph nodes
The lymphatic capillaries feed into larger and larger lymphatic vessels, and eventually empty into the bloodstream by a series of ducts. Along the way, the lymph travels through the lymph nodes, which are commonly found near the groin, armpits, neck, chest, and abdomen. A lymph node is one of the small, bean-shaped organs located throughout the lymphatic system. Cells of the immune system also use lymphatic vessels to return from interstitial spaces back into the circulation. Lymph nodes are connected by lymphatic vessels, and also act as “stations” for hosting immune cells so they can mount an immune response. Humans have about 500–600 lymph nodes throughout their body [Figure 20.29].

Figure 20.29: Anatomy of the Lymphatic System https://openstax.org/books/anatomy-and-physiology/pages/21-1-anatomy-of-the-lymphatic-and-immune-systems#fig-ch22_01_01 ]
A major difference between the lymphatic and cardiovascular systems is that lymph is not actively pumped by the heart, but is forced through the vessels by the movements of the body, the contraction of skeletal muscles during body movements, and breathing. Like veins, lymphatic vessels also have one-way valves that keep the lymph moving toward where they return to the circulatory system. These one-way valves are located fairly close to one another, and each one causes a bulge in the lymphatic vessel, giving the vessels a beaded appearance [FIGURE x.lymph.capillaries]. Lymph flows from lymphatic capillaries, through lymphatic vessels, and then is dumped into the circulatory system via the lymphatic ducts located at the junction of the jugular and subclavian veins in the neck.
Lymphatic Vessels, Trunks, and Ducts
As lymphatic capillaries empty into larger lymphatic vessels, these lymphatic vessels eventually merge to form even larger vessels known as lymphatic trunks. On the right side of the body, the right sides of the head, thorax, and right upper limb drain lymph fluid into the right subclavian vein via the right lymphatic duct [Figure x.lymph.ducts]. On the left side of the body, the remaining portions of the body drain into the larger thoracic duct, which drains into the left subclavian vein. The thoracic duct itself begins just beneath the diaphragm in the cisterna chyli, a sac-like chamber that receives lymph from the lower abdomen, pelvis, and lower limbs by way of the left and right lumbar trunks and the intestinal trunk.
Notice that the overall drainage system of the body is asymmetrical [Figure 20.30]. The right lymphatic duct receives lymph from only the upper right side of the body. The lymph from the rest of the body enters the bloodstream through the thoracic duct via all the remaining lymphatic trunks. In general, lymphatic vessels of the subcutaneous tissues of the skin, that is, the superficial lymphatics, follow the same routes as veins, whereas the deep lymphatic vessels of the viscera generally follow the paths of arteries.

Figure 20.30: Lymph Ducts https://openstax.org/books/anatomy-and-physiology/pages/21-1-anatomy-of-the-lymphatic-and-immune-systems#fig-ch22_01_03
20.4 Regulation of blood flow
![]() 20.4 Learning Outcomes
20.4 Learning Outcomes
- Discuss the mechanisms involved in the neural regulation of vascular homeostasis
- Describe the contribution of a variety of hormones to the renal regulation of blood pressure
- Identify the effects of exercise on vascular homeostasis
- Discuss how hypertension, hemorrhage, and circulatory shock affect vascular health
Although blood flows to all the tissues of your body, your body also needs to adjust and redistribute blood to different tissues based on situations you encounter in your daily life or things that disturb homeostasis in your body. Therefore, your body needs ways to regulate and control the flow of blood, and it does this in three primary ways: the nervous system, endocrine system, and autoregulation.
The nervous system controls
The primary areas of the nervous system that control vascular homeostasis are the cardiovascular centers in the brain that regulate both the heart and blood vessels. The limbic system and the autonomic nervous system also can affect and control cardiovascular homeostasis.
Brain Cardiovascular Centers
The cardiovascular centers are groups of neurons located in the medulla oblongata in the brain stem. Cardiovascular centers have powerful control over regulating blood pressure and flow. This cluster of neurons responds to changes in blood pressure as well as blood concentrations of oxygen, carbon dioxide, and hydrogen ions. The cardiovascular center contains three pairs of specialized neural centers that can function independently but are not anatomically distinct:
- Cardioaccelerator centers stimulate cardiac function by regulating heart rate and stroke volume via sympathetic stimulation from the cardiac accelerator nerve.
- Cardioinhibitor centers slow cardiac function by decreasing heart rate and stroke volume via parasympathetic stimulation from the vagus nerve.
- Vasomotor centers control vessel tone or contraction of the smooth muscle in the tunica media. Changes in diameter affect peripheral resistance, pressure, and flow, which affect cardiac output. The majority of these neurons act via the release of the neurotransmitter norepinephrine from sympathetic neurons.
There is also a small population of neurons that control vasodilation in the vessels of the brain and skeletal muscles by relaxing the smooth muscle fibers in the vessel tunics. Many of these neurons are cholinergic and release acetylcholine, which in turn stimulates vessel endothelial cells to release nitric oxide (NO), which causes vasodilation. Others release norepinephrine that binds to β2 receptors. A few neurons also release NO directly as a neurotransmitter.
Recall that mild stimulation of the skeletal muscles maintains muscle tone. A similar phenomenon occurs with vascular tone in vessels. As noted earlier, arterioles are normally partially constricted but can be stimulated to constrict further by vascular nerves (). With maximal stimulation, the radius of a vessel may be reduced to one-half of its resting state. For most arterioles, dilation requires suppression of sympathetic stimulation. When sympathetic stimulation and constriction are inhibited, an arteriole can expand by as much as 150 percent. As mentioned in this chapter, radius has a powerful effect on resistance and flow [link to heading: relationship between flow, pressure, and resistance] Therefore, sympathetic activity can dramatically affect resistance, pressure, and flow.
Baroreceptor Reflexes
Baroreceptors are specialized stretch receptors located within thin areas of blood vessels and heart chambers that respond to how much blood pressure stretches and distends these areas. Based on the amount of stretch they detect, baroreceptors will send impulses to the cardiovascular center, which in turn sends signals to regulate blood pressure. Vascular baroreceptors are found primarily in small bulges or pockets called sinuses within the aorta and carotid arteries. The are found in the walls of the just superior to the aortic valve, whereas the are in the base of the internal carotid arteries. There are also low-pressure baroreceptors located in the walls of the venae cavae and right atrium.
When blood pressure increases, the baroreceptors are stretched more tightly and fire off action potentials at a higher rate to the cardiovascular centers. At lower blood pressures, the degree of stretch is lower and the rate of firing is slower. When the cardiovascular center in the medulla oblongata receives input from baroreceptors, it triggers a reflex that tries to return blood pressure to normal homeostatic levels [Figure 20.31].
- When blood pressure is too high, the baroreceptors fire at a higher rate and trigger parasympathetic stimulation of the heart. This causes a decrease in heart rate and stroke volume, causing the cardiac output to decrease. Sympathetic stimulation of the peripheral arterioles will also decrease, resulting in vasodilation and less resistance. Combined, these activities cause blood pressure to fall.
- When blood pressure is too low, the rate of baroreceptor firing decreases. This will trigger an increase in sympathetic stimulation of the heart, causing the heart to beat faster and increase its stroke volume, causing the cardiac output to increase. It will also trigger sympathetic stimulation of the peripheral vessels, resulting in vasoconstriction. Combined, these activities cause blood pressure to rise.

Figure 20.31: Regulation Baroreflex https://openstax.org/books/anatomy-and-physiology/pages/20-4-homeostatic-regulation-of-the-vascular-system#fig-ch21_04_02
Baroreceptors are also located in the venae cavae and right atrium, and monitor the blood pressure of blood returning to the heart from systemic circulation. Normally, the amount of blood flowing out of the heart and into the aorta is the same as blood flow returning into the right atrium, so that blood does not accumulate in the heart, lungs, or systemic vessels. If blood is returning to the right atrium more rapidly than it is being ejected from the left ventricle, the atrial receptors will stimulate the cardiovascular centers to increase sympathetic firing and increase cardiac output until homeostasis is achieved. Accordingly, a decrease in right atrial pressure will cause the cardiovascular centers to decrease cardiac output. This mechanism is referred to as the (also Bainbridge reflex).
Chemoreceptor Reflexes
In addition to baroreceptors, chemoreceptors monitor blood levels of oxygen, carbon dioxide, and hydrogen ions (pH). Changes or problems with circulation can affect concentrations of these chemicals, therefore, chemoreceptors can send signals that adjust blood flow and maintain vascular homeostasis. Chemoreceptors monitoring the blood are located close to the baroreceptors in the aortic and carotid sinuses. They send signals to both the cardiovascular center and respiratory centers in the medulla oblongata.
Tissues consume oxygen and produce carbon dioxide and acids as waste products as part of cellular respiration, which provides energy that cells need to maintain homeostasis. For example, during exercise, oxygen levels fall and carbon dioxide levels rise as cells increase their rates of cellular respiration to meet the increased energy demand. This increased metabolism causes more hydrogen ions to be produced, causing the blood pH to drop. The chemoreceptors will respond to the increasing carbon dioxide and hydrogen ion levels (falling pH) by stimulating the cardioaccelerator and vasomotor centers, and suppressing cardioinhibitory centers. The increased cardioaccelerator and vasomotor center activity will increase cardiac output and constrict peripheral vessels to increase the perfusion of blood to the alveoli of the lungs so carbon dioxide can be excreted at a faster rate. An example of this can be seen in Table 20.4. One thing to note is that the integument has an increase in blood flow, which serves to help disperse heat caused by increased metabolism and activity, thereby maintaining temperature homeostasis during this process.
During exercise, the saturation of oxygen in the blood also drops due to the increased cellular activity, so the respiratory system also helps respond to changing metabolic demands. Chemoreceptors will stimulate respiratory centers to increase the rate of breathing and the volume of air that enters the lungs. This increased breathing will deliver more oxygen to the blood and also remove carbon dioxide from the blood at a faster rate.
| Organ | Resting
(mL/min) |
Mild exercise
(mL/min) |
Maximal exercise
(mL/min) |
| Skeletal muscle | 1200 | 4500 | 12,500 |
| Heart | 250 | 350 | 750 |
| Brain | 750 | 750 | 750 |
| Integument | 500 | 1500 | 1900 |
| Kidney | 1100 | 900 | 600 |
| Gastrointestinal | 1400 | 1100 | 600 |
| Others
(i.e., liver, spleen) |
600 | 400 | 400 |
| Total | 5800 | 9500 | 17,500 |
Table 20.4: Sympathetic Blood Flow Regulation from Openstax https://openstax.org/books/anatomy-and-physiology/pages/20-4-homeostatic-regulation-of-the-vascular-system#tbl-ch21_03 ]
Endocrine control
Many hormones work together with your nervous system to maintain blood pressure homeostasis if pressures become too high or low. Hormones have powerful effects on blood pressure, and several drugs that help with hypertension affect these hormones or receptors that respond to these hormones.
Epinephrine and norepinephrine
Hormones can also influence blood pressure and perfusion. During the “fight-or-flight” response, the sympathetic nervous system will trigger the release of epinephrine (also, adrenaline) and norepinephrine (also, noradrenaline) from the renal medulla. Both of these hormones will increase heart rate and stroke volume, thereby increasing cardiac output, which increases blood pressure. Epinephrine and norepinephrine also cause constriction of blood vessels that supply organs that are less important during a sympathetic response and redirect the blood flow to the heart, skeletal muscle, and other organs that help with sympathetic activity.
Antidiuretic Hormone
Antidiuretic hormone (ADH, also vasopressin) is produced by the cells in the hypothalamus and transported to the posterior pituitary where it is stored until released upon nervous stimulation. ADH is released from the posterior pituitary via nervous signals from the hypothalamus being stimulated by high blood osmolarity or release of angiotensin II. ADH targets cells in the kidneys and causes them to increase water reabsorption, which decreases fluid loss and, therefore, increases blood volume. This increased fluid retention will increase overall fluid levels and help restore blood volume. The increased blood volume caused by ADH will also increase blood pressure. In large amounts ADH may cause vasoconstriction, the reason for this hormone sometimes being referred to as vasopressin.
Aldosterone
Aldosterone is made in the adrenal cortex and as covered in the endocrine chapter this hormone is released in response to stimuli that affect blood volume and pressure, such as the release of angiotensin II. Aldosterone stimulates the absorption of Na+ and water in the kidneys, thus increasing plasma osmolarity, which causes the body to retain more fluid and increase blood volume and BP.
Renin-Angiotensin-Aldosterone System (RAAS)
The renin-angiotensin-aldosterone system raises blood volume and pressure through the hormones angiotensin II, aldosterone, and ADH. The liver makes and releases a protein called angiotensinogen into the blood, which is the starting protein from which angiotensin II is made. When the kidneys detect low BP or are activated by the sympathetic nervous system, it releases a protein called renin. Renin is an enzyme that converts angiotensinogen to angiotensin I, which does not have physiological effects on BP until it is converted. Angiotensin-converting enzyme (ACE) is located in the endothelium of the lungs and kidneys and converts angiotensin I into angiotensin II. As its name implies (“angio-”=blood vessel, “tensin”=tension), angiotensin II raises blood pressure. Angiotensin II has powerful effects on blood pressure by having multiple effects on the body, all of which increase blood pressure:
- Angiotensin II targets the kidneys and causes them to reabsorb more Na+ into the blood, thereby increasing plasma osmolarity, increasing water reabsorption, thus increasing BP.
- Angiotensin II targets the hypothalamus and stimulates thirst, increasing water intake, thus increasing body fluids and BP.
- Angiotensin II stimulates the release of ADH from the posterior pituitary, which decreases urine production and increases fluid retention and BP.
- Angiotensin II causes vasoconstriction of systemic arterioles, which increases BP due to the increased resistance.
- Angiotensin II acts on the adrenal cortex to release aldosterone, which has the overall effect of increasing BP.
Antihypertensives are a class of drugs that are used to control hypertension, and many of them affect angiotensin II and its receptors due to the powerful effects angiotensin II has on BP. Angiotensin-converting enzyme inhibitors (ACE inhibitors) are a type of drug that block angiotensin-converting enzymes, which would prevent the formation of angiotensin II, thus lowering BP. Angiotensin II receptor blockers (ARBs) are a type of drug that prevent angiotensin II from binding to its receptors, which also lowers BP.
Erythropoietin
Erythropoietin (EPO) is released by the kidneys in response to decreased blood flow or blood oxygen levels. EPO stimulates the production of RBCs within the bone marrow to increase oxygen transport in response to the low flow of oxygen. RBCs alone make up over 40 percent of blood volume, and their amount affects viscosity, resistance, pressure, and flow. Increased amounts of RBCs will thereby increase blood volume and BP. In addition, EPO is a vasoconstrictor, which also increases BP.
Atrial Natriuretic Peptide
Atrial natriuretic peptide (ANP) (also atrial natriuretic hormone) is secreted by cells in the atria of the heart. ANP is secreted when blood volume is high enough to cause extreme stretching of the cardiac cells. B-type natriuretic hormone (BNP) is a related hormone produced by cells in the ventricles of the heart. Unlike the other hormones in this chapter, ANP & BNP oppose the effects of angiotensin II. True to their name (“natri-” = sodium; “uretic” = urine), natriuretic peptides promote the loss of sodium and water from the kidneys and suppress renin, aldosterone, and ADH production and release. This leads to an overall loss in blood volume and pressure due to the loss of fluid from the body.
Autoregulation
Precapillary sphincters control the flow of blood into capillary beds. Relaxation of these sphincter muscles allows blood to flow into capillaries maximizing perfusion. Contraction of the sphincters bypasses the bed, pushing flow through the thoroughfare channel. Local vasodilators increase blood flow to adjust to metabolic activity changes. An increase in carbon dioxide, lactic acid, and H+ and K+ will stimulate capillary sphincters to relax and allow flow into the capillary bed and surrounding tissues to flush out these waste products. A decline in oxygen and other nutrients may also stimulate capillary sphincter relaxation and an increase in perfusion.
Chemicals released in response to tissue damage or the body’s immune system may also alter blood flow to local areas. Vasodilators include nitric oxide, histamine, and bradykinin. These may be released in response to trauma, allergies, infection, or even exercise. Local vasoconstrictors include prostaglandins and thromboxanes. These are released in response to tissue damage and help prevent blood loss.
 |
 |
| Normal blood vessel (L) Vs. Vasodilation (R) | Vasoconstriction – Constricted blood vessel |
Figure 20.32 x.regulation.vasodilators Illustration of release or build of vasodilators and constrictors influence blood flow
Myogenic response
involves the smooth muscle in blood vessel walls. In addition to the effects of vasodilators and vasoconstrictors, these tissues keep local blood flow relatively constant by responding to the local BP. If systemic blood pressure rises & more blood enters an arteriole, the walls will stretch. Smooth muscle cells respond by contracting. Contraction reduces the lumen size, limiting blood volume thus returning local flow to original levels. If systemic BP decreases, then the amount of blood decreases as well. Then there will be less stretch causing smooth muscle of vessel walls to relax. Relaxation will increase lumen size and return local blood flow to original levels.

Figure 20.33: Myogenic Regulation.Illustration showing constriction and relaxation in response to BP changes
![]() Local Issue
Local Issue
Exercise in hot, humid environments and hypovolemic shock
Physiological response to exercise is a complex relationship between the environment and thermal homeostasis, as modulated by heat-regulating mechanisms. Thermoregulation is controlled by the hypothalamus and heat-regulating mechanisms are activated when: peripheral thermal receptors are stimulated and changes in the temperature of blood flowing through the brain are detected. In response to hyperthermia, the body dissipates heat through radiation, conduction, convention, and evaporation. Heat loss via evaporation of sweat is key for heat loss when radiant heat & environment temperatures are greater than body temperature. But in Hawaiʻi, prolonged physical activity in the hot environment may lead to excessive sweating, and the subsequent loss of water is reflected by a decrease in circulating blood in the body resulting in low blood volume. Low blood volume due to dehydration can result in hypovolemic shock. Symptoms of hypovolemic shock include confusion, cool and clammy skin, pale skin, rapid breathing, and, in severe cases, unconsciousness. It is important to take precautions when exercising in Hawaiʻi — exercise in the early morning or late afternoon hours, wear appropriate clothing for thermoregulation, and, if new to Hawaiʻi, wait several weeks before exercising so your body acclimates to the effects of warm weather.
20.5 Circulatory Pathways
![]() 20.5 Learning Outcomes
20.5 Learning Outcomes
- Identify the vessels through which blood travels within the , beginning from the right ventricle of the heart and ending at the left atrium
- Create a flowchart showing the major systemic arteries through which blood travels from the aorta and its major branches to the most significant arteries feeding into the right and left upper and lower limbs.
- Create a flowchart showing the major systemic veins through which blood travels from the feet to the right atrium of the heart
Remember, arteries carry blood away from the heart and veins carry blood to the heart. The circulatory system can be divided into two subsystems; pulmonary and systemic circulation. In the pulmonary circulatory system, arteries carry oxygen-depleted blood from the right ventricle to the lungs where gas exchange occurs. The blood, now oxygen saturated, is returned to the left side of the heart via . For the systemic circulation, arteries carry oxygen saturated blood away from the left side of the heart to the capillary beds throughout the body. Perfusion, including gas exchange, occurs in these beds. Oxygen-depleted blood returns to the venous side of these beds and returns to the heart through the larger veins. Therefore, pulmonary arteries carry oxygenated blood in the systemic circulatory system whereas pulmonary arteries carry oxygen-depleted blood in the pulmonary system.

Figure 20.34: Cardiovascular Circulation Illustration showing oxygenated vs deoxygenated blood in the pulmonary and systemic systems https://openstax.org/books/anatomy-and-physiology/pages/20-1-structure-and-function-of-blood-vessels#fig-ch21_01_01
Aorta
The aorta is the largest artery in the human body. It extends from the left ventricle of the heart, ascending superiorly before bending and descending inferiorly through the thoracic and abdominal cavities. Branching from the ascending aorta are the left and right coronary arteries that feed the heart wall tissues. Where the aorta bends it is referred to as the . Three main branches emerge from the aorta arch. The brachiocephalic trunk serves the right side of the body. This trunk bifurcates into the right common carotid and the right subclavian arteries. On the left side of the body, there isn’t a brachiocephalic trunk. Instead, the left common carotid artery and the left branch directly from the aortic arch. Both the left and right common carotid arteries deliver blood to the head. The left and right subclavian arteries serve the arms and some thoracic tissues.

Figure 20.35: Aorta The aorta has distinct regions, including the ascending aorta, aortic arch, and the , which includes the thoracic and abdominal regions.
As the aortic arch curves inferiorly it becomes the descending aorta. It is first the descending serving the thoracic wall and organs. The aorta then pierces the diaphragm becoming the descending feeding the wall and organs of the abdomen. Near vertebrae L4 it splits into the left and right common iliac arteries. Each of these splits into internal iliac arteries feeding the pelvis and external iliac arteries serving the lower limbs.
From these major arteries all other named systemic arteries branch eventually bifurcate into smaller and smaller vessels that eventually supply capillary beds. From capillary beds, venules merge into small veins. These veins merge to form the larger named venous vessels. The largest veins, the superior and , return systemic blood to the right atrium of the heart. The forms by the merger of the left and right s which drain the head, neck, upper limbs, and parts of the thoracic and abdominal walls. The inferior vena cava forms from merging veins inferior to the diaphragm. This major vessel returns blood from the lower limbs, pelvis, perineum, and abdominal tissues. Separate from the vena cavas, the coronary sinus returns venous blood from coronary circulation back to the right atrium.

Figure 20.36: Arteries and Veins: The arteries of the body, indicated in red, start at the aortic arch and branch to supply the organs and muscles of the body with oxygenated blood. The veins of the body, indicated in blue, return blood to the heart. The pulmonary arteries are blue to reflect the fact that they are deoxygenated, and the pulmonary veins are red to reflect that they are oxygenated. (credit: OS Concepts of Biology, modification of work by Mariana Ruiz Villareal)
 |
 |
| Systemic Arteries: The major systemic arteries shown here deliver oxygenated blood throughout the body. | Major Systemic Veins of the Body: The major systemic veins of the body are shown here in an anterior view. |
Figure 20.37: Systemic Arteries and Veins

Figure 20.38: Interaction of the Circulatory System with Other Systems

Figure 20.39: Coronary Circulation

Figure 20.40: Internal Structures of the Heart: This anterior view of the heart shows the four chambers, the major vessels and their early branches, as well as the valves. The presence of the pulmonary trunk and aorta covers the interatrial septum, and the atrioventricular septum is cut away to show the atrioventricular valves.
Head
The common carotid arteries supply most of the blood delivered to the head. The left and right common carotids flank the trachea dividing into the external and internal branches.
External carotids feed structures outside of the skull, whereas the internal carotid feeds deeper tissues. Branches from the subclavian artery also feed some organs of the head. The serves the brain. The thyrocervical trunk serves the thyroid gland, parts of the neck in addition to regions of the shoulder. The costocervical trunk serves deeper neck tissues and areas in the upper intercostals.
Branching from each is the superior thyroid artery serving the thyroid gland and larynx, the ascending pharyngeal artery serving the pharynx, the lingual artery feeding the tongue, the facial artery, the occipital artery for the posterior scalp, posterior auricular artery serving the ears and scalp, the superficial temporal artery for the parotid gland and scalp and the maxillary artery for the teeth, gums, nasal cavity, meninges and muscles for mastication.
The internal carotid arteries branch after entering the skull. The anterior and branches serve the brain. The feeds the eyes and surrounding tissues. The vertebral branch from the subclavian artery passes through the transverse foramina of the cervical vertebrae, enters the skull via the foramen magnum and merge to form the unpaired . The basilar artery then divides into the posterior cerebral arteries to feed the dorsal cerebrum. Helping to equalize the pressure in the brain and ensure blood flow are arterial anastomoses nearby the sella turcica. These anastomoses, known as the , form by the merging of the posterior cerebral, posterior communicating, internal carotid, anterior cerebral & anterior communicating arteries.

Figure 20.41: Arteries Supplying the Head and Neck The common carotid artery gives rise to the external and internal carotid arteries. The external carotid artery remains superficial and gives rise to many arteries of the head. The first forms the carotid sinus and then reaches the brain via the carotid canal and carotid foramen, emerging into the cranium via the foramen lacerum. The vertebral artery branches from the subclavian artery and passes through the transverse foramen in the cervical vertebrae, entering the base of the skull at the vertebral foramen. The subclavian artery continues toward the arm as the .
 |
 |
| Arteries Serving the Brain This inferior view shows the network of arteries serving the brain. The structure is referred to as the arterial circle or circle of Willis. | Circle of Willis The blood supply to the brain enters through the internal carotid arteries and the vertebral arteries, eventually giving rise to the circle of Willis. |
20.42 Arteries Serving the Brain This inferior view shows the network of arteries serving the brain. The structure is referred to as the or circle of Willis.
Venous drainage of the head
Three primary veins drain the head and neck. The vertebral and s empty into the subclavian vein. The internal jugular joins the subclavian to form the brachiocephalic vein. The external jugular vein drains superficial head and neck structures. The cranial cavity is drained in part by the s but most cranial blood drains into the dural venous sinuses which are large modified veins between layers of dura mater. These sinuses also drain excess cerebrospinal fluid. The sinuses drain primarily into the s. The dural sinuses consist of several regional parts including the and the superior sagittal, straight, cavernous, the , occipital, transverse and .

Figure 20.43: Veins of the Head and Neck This left lateral view shows the veins of the head and neck, including the intercranial sinuses.

Figure 20.44: Dural Sinuses and Veins Blood drains from the brain through a series of sinuses that connect to the jugular veins.
Trunk
Arterial
Arterial supply of the trunk comes from the branches of the descending aorta and the internal thoracic, inferior epigastric and supreme intercostal arteries. Posterior intercostal arteries 3-11 branch from the thoracic aorta and anastomose with the anterior intercostal arteries. Serving the posterolateral abdominal wall are 4-5 pairs of that branch from the abdominal aorta. At the distal end, the unpaired bifurcates from the aorta within the pelvis and serves the sacrum and coccyx. The serves the anterior thoracic wall and mammary glands. It emerges from the subclavian artery and branches into six anterior intercostal arteries to serve the intercostal spaces and the musculophrenic artery which further divides into some anterior intercostal arteries (7–9). Then the internal thoracic artery becomes the superior epigastric artery to feed the superior abdominal wall. The inferior epigastric artery serves the inferior abdominal wall and emerges from the external iliac eventually forming an anastomosis with the superior epigastric artery. Supreme intercostal arteries branch from the costocervical trunk and then divide into the 1st-2nd posterior intercostal arteries.

Figure 20.45: Arteries of the Thoracic and Abdominal Regions The thoracic aorta gives rise to the arteries of the visceral and .
Venous
The receives blood from anterior intercostal, musculophrenic, and superior epigastric veins and then delivers it to the brachiocephalic vein. The inferior epigastric vein merges with the . The 1st and 2nd posterior s merge with supreme intercostal veins, draining into the brachiocephalic vein.
The azygos system of veins receives blood from lumbar & posterior intercostal veins. The term azygous means unpaired; therefore, the azygos system is composed of unpaired venous vessels. The hemiazygos and accessory s occur on the left side of the body, whereas the occurs only on the right. These drain into the superior vena cava.

Figure 20.46: Veins of the Thoracic and Abdominal Regions: Veins of the thoracic and abdominal regions drain blood from the area above the diaphragm, returning it to the right atrium via the superior vena cava.
Specific organs
Lungs
The lungs are fed by bronchial arteries that emerge as tiny branches off the descending thoracic aorta. These serve the bronchi and bronchioles. s drain into the azygos and pulmonary veins.

Figure 20.47: Pulmonary Circuit Blood exiting from the right ventricle flows into the pulmonary trunk, which bifurcates into the two pulmonary arteries. These vessels branch to supply blood to the pulmonary capillaries, where gas exchange occurs within the lung alveoli. Blood returns via the pulmonary veins to the left atrium.
Esophagus
The esophageal arteries emerge from several origins. Small branches of the inferior thyroid artery serve the upper esophageal region. The middle region is served by esophageal arteries emerging from the descending thoracic aorta. The inferior region is served by branches from the . The s drain into the azygos or left gastric vein.
 |
 |
| Esophagus: The position and relation of the esophagus in the cervical region and in the posterior mediastinum. Seen from behind. | Relations of the aorta, trachea, esophagus and other structures of and around the heart. Anterior view. Structures are appearing as transparent in order to visualize overlapping structures, but are not transparent in reality. |
 |
|
 |
|
Figure 20.48: Esophageal Region
Diaphragm
The diaphragm is served by several arteries and veins. The superior phrenic arteries emerge from descending thoracic aorta, the inferior phrenic arteries emerge from descending abdominal aorta and the musculophrenic and pericardiacophrenic arteries arise from the internal thoracic artery. The diaphragm is drained by the superior phrenic and inferior s which drain into the inferior vena cava and the musculophrenic vein which drains to internal thoracic veins.
 |
|
| Muscles of the Diaphragm | |
 |
|
  |
Figure 20.49 Diaphragm
GI tract
Blood supply to the gastrointestinal tract comes from the abdominal aorta emerging as three unpaired arteries: the and the superior and inferior mesenteric arteries.
Celiac trunk
The celiac trunk is located just inferior to the diaphragm and has three branches. The left gastric artery serves part of the stomach and esophagus. The serves the spleen (hence its name) and parts of the stomach and pancreas. The third branch is the and has two main branches: the and the gastroduodenal arteries. The hepatic artery proper serves the liver (hence its name), gallbladder, and part of the stomach. The gastroduodenal artery also serves part of the stomach and pancreas, but also the duodenum.
 |
 |
| Pancreas/splenic arteries and veins. Posterior view |
A diagram showing the arterial blood supply to the stomach and the spleen. |
 |
|
| The image shows the celiac trunk, its major branches and distribution to the viscera of the upper abdomen; derivatives of the embryonic foregut. | |
Figure 20.50: The Celiac Trunk
Superior mesenteric artery
is located immediately inferior to the celiac trunk. It branches into the intestinal arteries serving the jejunum and ileum, the middle colic artery feeding most of the transverse colon, the right colic artery serving the ascending colon, and the ileocolic artery feeding the ileum, cecum, and appendix.
Inferior mesenteric artery
Located just above the bifurcation of the aorta is the . It has three branches: the left colic, sigmoid, and superior rectal arteries. The left colic serves the distal transverse colon and descending colon, the sigmoid arteries serve parts of descending colon and sigmoid colon, and the superior rectal artery serves the rectum.
 |
 |
 |
| Layers of the Alimentary Canal The wall of the alimentary canal has four basic tissue layers: the mucosa, submucosa, muscularis, and serosa. | Superior mesenteric artery | Inferior mesenteric artery |
Figure 20.51: Superior and Inferior Mesenteric Arteries
Hepatic portal system
Blood from the digestive organs are sent to the liver. Some digested nutrients may be processed. The liver also helps to remove harmful agents. This system of venous return from the GI tract is called the . This system consists of three main veins that drain into the hepatic portal vein: the splenic vein, the inferior mesenteric vein, and the superior mesenteric vein. The delivers blood to the liver sinusoids. Hepatic blood is drained into the inferior vena cava.

Figure 20:52: Hepatic Portal System The liver receives blood from the normal systemic circulation via the hepatic artery. It also receives and processes blood from other organs, delivered via the veins of the hepatic portal system. All blood exits the liver via the hepatic vein, which delivers the blood to the inferior vena cava. (Different colors are used to help distinguish among the different vessels in the system.)
 |
 |
| (A) The schematic shows an adult liver (red), with the gall bladder and extra hepatic ducts (green), in relation to the stomach and intestine (yellow). The extra hepatic duct system consists of the hepatic ducts (hd), which drain bile from the liver into the common hepatic duct (chd) to the gall bladder via the cystic duct (cd) and into the duodenum through the common bile duct (cbd). (B) A schematic of the cellular architecture of the liver showing the hepatocytes (pink) arranged in hepatic plates separated by sinusoid spaces radiating around a central vein. Bile canaliculi on the surface of adjoining hepatocytes drain bile into the bile ducts (green), which run parallel to portal veins (blue) and hepatic arteries (red) to form the “portal triad”. (Panel B is adapted with permission from Bloom and Fawcett: A Text Book of Histology 10th Edition). | A labelled diagram of the cells and structures of a liver lobule in mammals. |
Figure 20:53: Hepatic sinusoids
Posterior abdominal organs, pelvis and perineum
A middle suprarenal artery supplies each adrenal gland that is on top of the kidneys while a supplies each kidney. A supplies the gonads. The middle suprarenal, renal, and gonadal arteries are branches of the descending aorta and are drained by veins of the same name.
The right and left common iliacs divide into internal & external iliac arteries. The is the primary arterial blood supply to the pelvic region and has several branches. The superior gluteal artery branch serves the gluteus medius and minimus. The inferior gluteal artery branch serves the gluteus maximus. The bladder is fed by the superior vesical artery. The middle rectal artery serves the rectum. Vaginal and uterine arteries serve the vagina and uterus, respectively. The internal pudendal artery feeds the anal canal and perineum. The medial thigh muscles are fed by the obturator artery. Fetal umbilical arteries become the median umbilical ligaments. Venous drainage of the pelvic and perineum regions are by veins named similar to their arterial counterparts. They merge with the , which merges with the .
 |
 |
| Posterior Organs on the right side of the diagram. Full Diagram shows: 1: diaphragm – 2: liver – 3: stomach – 4: bladder – 5: pubic bone – 6: vagina – 7 : pancreas – 8: duodenum – 9: transverse colon – 10 : small intestine – 11 : uterus – 12 : rectum | Pancreas |
Figure 20:54 Illustration of the Posterior abdominal organs

Figure 20:55 Pelvis and perineum vessels
Upper Limbs
Both the upper and lower limbs receive blood from one main artery that bifurcates at the elbow or knee. Both the arterial and venous vasculature of the limbs contain many arches. The venous systems include both superficial and deep networks of veins.
Arteries
Remember that the left subclavian artery comes off the aortic arch whereas the right subclavian artery comes off the brachiocephalic trunk. The subclavian continues on as the axillary artery after the vessel passes beyond the first rib. The axillary artery feeds the axilla, chest wall, shoulder, and humerus and becomes the brachial artery as it passes beyond the teres major. The deep brachial artery branches from the brachial artery and supplies blood to most arm muscles. The radial and ulnar arteries are divisions of the brachial artery and supply the forearm and wrist. These anastomose and form two arterial arches: the deep palmar arch (primarily from the radial) and the superficial palmar arch (primarily from the ulnar). emerge from these arches to supply fingers.

Figure 20.56: Major Arteries Serving the Thorax and Upper Limb
Veins
Superficial venous drainage can be highly variable among individuals. It includes a dorsal venous network (arch) on the hand dorsum that drains into the medial and lateral cephalic vein. Blood is then delivered to the . The connects cephalic and basilic veins in the cubital region and is a common site for venipuncture.
Deep venous drainage uses the and superficial which drain into radial and s running parallel to their counterpart arteries. s, formed by the merger of radial and ulnar veins, also travel with brachial arteries. The axillary vein forms from the brachial and basilic vein merger. At the lateral border of the first rib, the axillary becomes the subclavian vein which merges with the internal jugular to form the brachiocephalic vein.

Figure 20.57: Veins of the Upper Limb
![]() Retrieval Practice
Retrieval Practice
Learning Arteries and Veins
Optimize your learning of the vessels by referring back to the Introduction Chapter’s Regional Names section and an illustration of the Regions of the Human Body. You will observe the names of regions such as axilla and brachium. Notice how many of those regional terms are used in the arteries and veins of the body. Get a solid understanding of the Introduction Chapter regions, and the associated root words, and it will make remembering vessel names much more meaningful…and easier!
Are you done reviewing the Introduction Chapter’s Regions of the Human Body illustration and relating it to this chapter’s circulatory pathways (naming arteries and veins)? Now it is time for your retrieval practice, informed by your fresh memories of regional terms. Take another look at the upper limb arteries and veins paragraphs and create a list of the vessels (e.g., digital artery, basilic vein) that are bolded in the paragraphs. Put away the textbook and create a very rough sketch of the arm and hand and all the vessels on your list, labeling each vessel (artery and vein). When you have finished, refer back to the artery and vein figures of the arm and hand and correct your work. Try this technique for all the other arteries and veins in this chapter.
Lower Limbs
Arteries
The is the main supply to the lower limbs. It begins as a branch of the and becomes the as it passes the inguinal ligament. A branch of the femoral artery forms the traveling posteromedially serving the hip joint and many thigh muscles. The is the continuation of the femoral artery in the popliteal fossa supplying the knee joint and regional muscles. The popliteal divides into anterior and posterior tibial arteries.
The serves the anterior crural region and continues on as the as it crosses the ankle. The feeds the posterior leg along with its major, branch the fibular artery which serves the lateral leg. Medial and lateral plantar arteries serve the plantar side of the foot and are a continuation of the posterior tibial artery. The plantar arterial arch of the foot forms from merger of the dorsalis pedis and a branch of . Extending from the are the digital arteries feeding the toes.

Figure 20.58: Major Arteries Serving the Lower Limb Major arteries serving the lower limb are shown in anterior and posterior views.
Veins
Superficial veins of the lower leg include the and the great saphenous and s. The dorsal venous arch drains the dorsum of the foot and delivers the blood to the great and small saphenous veins. The originates in the medial ankle, extends along the medial surface of the entire lower limb, and drains into the . The small saphenous vein extends adjacent to the lateral ankle, and travels along the posterior calf, draining into the .
The deeper veins of the lower limb include the paired medial and lateral which drain the digital veins and other deep veins of the foot. The s drain the plantar veins and s. The s drain deep veins of the foot and ankle. The popliteal vein forms from the merger of anterior and posterior tibial veins becoming the femoral vein in anterior thigh and the external iliac vein superior to inguinal ligament. The common iliac forms from merged external and internal iliac veins.

Figure 20.59: Major Veins Serving the Lower Limbs Anterior and posterior views show the major veins that drain the lower limb into the inferior vena cava.
![]() Deep Dive
Deep Dive
Trace the movement of a RBC through the vasculature as it travels from the capillary bed of the left thumb to the capillary bed of the right thumb.

Chapter Summary
References
- Blood pressures
- Capillary Exchange
- CHP
- https://journals.physiology.org/doi/pdf/10.1152/advan.00084.2006
- “Although the reported values differ, [interstitial hydrostatic] pressures probably range from 8 mmHg in the lungs to 3 or 2 mmHg in the subcutaneous tissue to 0, 1, and 2 mmHg in the liver and kidneys or 6 mmHg in the brain (4, 6)”
- https://journals.physiology.org/doi/pdf/10.1152/advan.00084.2006
- CHP

Key Terms
abdominal aorta
portion of the aorta inferior to the aortic hiatus and superior to the common iliac
arteries
angiogenesis
development of new blood vessels from existing vessels
anterior tibial artery
branches from the popliteal artery; supplies blood to the anterior tibial region; becomes the dorsalis pedis artery
anterior tibial vein
forms from the dorsal venous arch; drains the area near the tibialis anterior muscle and leads to the popliteal vein
aorta
largest artery in the body, originating from the left ventricle and descending to the abdominal region where it bifurcates into the common iliac arteries at the level of the fourth lumbar vertebra; arteries originating from the aorta distribute blood to virtually all tissues of the body
aortic arch
arc that connects the ascending aorta to the descending aorta; ends at the intervertebral disk between the fourth and fifth thoracic vertebrae
aortic sinuses
small pockets in the ascending aorta near the aortic valve that are the locations of the baroreceptors (stretch receptors) and chemoreceptors that trigger a reflex that aids in the regulation of vascular homeostasis
arterial circle
(also, circle of Willis) anastomosis located at the base of the brain that ensures continual blood supply; formed from branches of the internal carotid and vertebral arteries; supplies blood to the brain
arteriole
(also, resistance vessel) very small artery that leads to a capillary
arteriovenous anastomosis
short vessel connecting an arteriole directly to a venule and bypassing the capillary beds
artery
blood vessel that conducts blood away from the heart; may be a conducting or distributing vessel
ascending aorta
initial portion of the aorta, rising from the left ventricle for a distance of approximately 5 cm
atrial reflex
mechanism for maintaining vascular homeostasis involving atrial baroreceptors: if blood is returning to the right atrium more rapidly than it is being ejected from the left ventricle, the atrial receptors will stimulate the cardiovascular centers to increase sympathetic firing and increase cardiac output until the situation is reversed; the opposite is also true
axillary artery
continuation of the subclavian artery as it penetrates the body wall and enters the axillary region; supplies blood to the region near the head of the humerus (humeral circumflex arteries); the majority of the vessel continues into the brachium and becomes the brachial artery
axillary vein
major vein in the axillary region; drains the upper limb and becomes the subclavian vein
azygos vein
originates in the lumbar region and passes through the diaphragm into the thoracic cavity on the right side of the vertebral column; drains blood from the intercostal veins, esophageal veins, bronchial veins, and other veins draining the mediastinal region; leads to the superior vena cava
basilar artery
formed from the fusion of the two vertebral arteries; sends branches to the cerebellum, brain stem, and the posterior cerebral arteries; the main blood supply to the brain stem
basilic vein
superficial vein of the arm that arises from the palmar venous arches, intersects with the median cubital vein, parallels the ulnar vein, and continues into the upper arm; along with the brachial vein, it leads to the axillary vein
blood colloidal osmotic pressure (BCOP)
pressure exerted by colloids suspended in blood within a vessel; a primary determinant is the presence of plasma proteins
blood flow
movement of blood through a vessel, tissue, or organ that is usually expressed in terms of volume per unit of time
blood hydrostatic pressure (BHP)
force blood exerts against the walls of a blood vessel or heart chamber
blood pressure
force exerted by the blood against the wall of a vessel or heart chamber; can be described with the more generic term hydrostatic pressure
brachial artery
continuation of the axillary artery in the brachium; supplies blood to much of the brachial region; gives off several smaller branches that provide blood to the posterior surface of the arm in the region of the elbow; bifurcates into the radial and ulnar arteries at the coronoid fossa
brachial vein
deeper vein of the arm that forms from the radial and ulnar veins in the lower arm; leads to the axillary vein
brachiocephalic vein
one of a pair of veins that form from a fusion of the external and internal jugular veins and the subclavian vein; subclavian, external and internal jugulars, vertebral, and internal thoracic veins lead to it; drains the upper thoracic region and flows into the superior vena cava
bronchial vein
drains the systemic circulation from the lungs and leads to the azygos vein
capacitance
ability of a vein to distend and store blood
capillary
smallest of blood vessels where physical exchange occurs between the blood and tissue cells surrounded by interstitial fluid
capillary bed
network of 10–100 capillaries connecting arterioles to venules
capillary hydrostatic pressure (CHP)
force blood exerts against a capillary
carotid sinuses
small pockets near the base of the internal carotid arteries that are the locations of the baroreceptors and chemoreceptors that trigger a reflex that aids in the regulation of vascular homeostasis
celiac trunk
(also, celiac artery) major branch of the abdominal aorta; gives rise to the left gastric artery, the splenic artery, and the common hepatic artery that forms the hepatic artery to the liver, the right gastric artery to the stomach, and the cystic artery to the gallbladder
cephalic vein
superficial vessel in the upper arm; leads to the axillary vein
circle of Willis
(also, arterial circle) anastomosis located at the base of the brain that ensures continual blood supply; formed from branches of the internal carotid and vertebral arteries; supplies blood to the brain
circulatory shock
also simply called shock; a life-threatening medical condition in which the circulatory system is unable to supply enough blood flow to provide adequate oxygen and other nutrients to the tissues to maintain cellular metabolism
common carotid artery
right common carotid artery arises from the brachiocephalic artery, and the left common carotid arises from the aortic arch; gives rise to the external and internal carotid arteries; supplies the respective sides of the head and neck
common hepatic artery
branch of the celiac trunk that forms the hepatic artery, the right gastric artery, and the cystic artery
common iliac artery
branch of the aorta that leads to the internal and external iliac arteries
common iliac vein
one of a pair of veins that flows into the inferior vena cava at the level of L5; the left common iliac vein drains the sacral region; divides into external and internal iliac veins near the inferior portion of the sacroiliac joint
compliance
degree to which a blood vessel can stretch as opposed to being rigid
deep femoral artery
branch of the femoral artery; gives rise to the lateral circumflex arteries
descending aorta
portion of the aorta that continues downward past the end of the aortic arch; subdivided into the thoracic aorta and the abdominal aorta
diastolic pressure
lower number recorded when measuring arterial blood pressure; represents the minimal value corresponding to the pressure that remains during ventricular relaxation
digital arteries
formed from the superficial and deep palmar arches; supply blood to the digits
digital veins
drain the digits and feed into the palmar arches of the hand and dorsal venous arch of the foot
dorsal venous arch
drains blood from digital veins and vessels on the superior surface of the foot
dorsalis pedis artery
forms from the anterior tibial artery; branches repeatedly to supply blood to the tarsal and dorsal regions of the foot
elastic artery
(also, conducting artery) artery with abundant elastic fibers located closer to the heart, which maintains the pressure gradient and conducts blood to smaller branches
esophageal vein
drains the inferior portions of the esophagus and leads to the azygos vein
external carotid artery
arises from the common carotid artery; supplies blood to numerous structures within the face, lower jaw, neck, esophagus, and larynx
external iliac artery
branch of the common iliac artery that leaves the body cavity and becomes a femoral artery; supplies blood to the lower limbs
external iliac vein
formed when the femoral vein passes into the body cavity; drains the legs and leads to the common iliac vein
external jugular vein
one of a pair of major veins located in the superficial neck region that drains blood from the more superficial portions of the head, scalp, and cranial regions, and leads to the subclavian vein
femoral artery
continuation of the external iliac artery after it passes through the body cavity; divides into several smaller branches, the lateral deep femoral artery, and the genicular artery; becomes the popliteal artery as it passes posterior to the knee
femoral vein
drains the upper leg; receives blood from the great saphenous vein, the deep femoral vein, and the femoral circumflex vein; becomes the external iliac vein when it crosses the body wall
fibular vein
drains the muscles and integument near the fibula and leads to the popliteal vein
filtration
in the cardiovascular system, the movement of material from a capillary into the interstitial fluid, moving from an area of higher pressure to lower pressure
gonadal artery
branch of the abdominal aorta; supplies blood to the gonads or reproductive organs; also described as ovarian arteries or testicular arteries, depending upon the sex of the individual
great cerebral vein
receives most of the smaller vessels from the inferior cerebral veins and leads to the straight sinus
great saphenous vein
prominent surface vessel located on the medial surface of the leg and thigh; drains the superficial portions of these areas and leads to the femoral vein
hemiazygos vein
smaller vein complementary to the azygos vein; drains the esophageal veins from the esophagus and the left intercostal veins, and leads to the brachiocephalic vein via the superior intercostal vein
hepatic artery proper
branch of the common hepatic artery; supplies systemic blood to the liver
hepatic portal system
specialized circulatory pathway that carries blood from digestive organs to the liver for processing before being sent to the systemic circulation
hepatic vein
drains systemic blood from the liver and flows into the inferior vena cava
hypertension
chronic and persistent blood pressure measurements of 140/90 mm Hg or above
hypervolemia
abnormally high levels of fluid and blood within the body
hypovolemia
abnormally low levels of fluid and blood within the body
hypovolemic shock
type of circulatory shock caused by excessive loss of blood volume due to hemorrhage or possibly dehydration
hypoxia
lack of oxygen supply to the tissues
inferior mesenteric artery
branch of the abdominal aorta; supplies blood to the distal segment of the large intestine and rectum
inferior vena cava
large systemic vein that drains blood from areas largely inferior to the diaphragm; empties into the right atrium
intercostal vein
drains the muscles of the thoracic wall and leads to the azygos vein
internal carotid artery
arises from the common carotid artery and begins with the carotid sinus; goes through the carotid canal of the temporal bone to the base of the brain; combines with branches of the vertebral artery forming the arterial circle; supplies blood to the brain
internal iliac artery
branch from the common iliac arteries; supplies blood to the urinary bladder, walls of the pelvis, external genitalia, and the medial portion of the femoral region; in females, also provide blood to the uterus and vagina
internal iliac vein
drains the pelvic organs and integument; formed from several smaller veins in the region; leads to the common iliac vein
internal jugular vein
one of a pair of major veins located in the neck region that passes through the jugular foramen and canal, flows parallel to the common carotid artery that is more or less its counterpart; primarily drains blood from the brain, receives the superficial facial vein, and empties into the subclavian vein
internal thoracic artery
(also, mammary artery) arises from the subclavian artery; supplies blood to the thymus, pericardium of the heart, and the anterior chest wall
internal thoracic vein
(also, internal mammary vein) drains the anterior surface of the chest wall and leads to the brachiocephalic vein
interstitial fluid colloidal osmotic pressure (IFCOP)
pressure exerted by the colloids within the interstitial fluid
interstitial fluid hydrostatic pressure (IFHP)
force exerted by the fluid in the tissue spaces
ischemia
insufficient blood flow to the tissues
Korotkoff sounds
noises created by turbulent blood flow through the vessels
lateral plantar artery
arises from the bifurcation of the posterior tibial arteries; supplies blood to the lateral plantar surfaces of the foot
left gastric artery
branch of the celiac trunk; supplies blood to the stomach
lumbar arteries
branches of the abdominal aorta; supply blood to the lumbar region, the abdominal wall, and spinal cord
lumen
interior of a tubular structure such as a blood vessel or a portion of the alimentary canal through which blood, chyme, or other substances travel
mean arterial pressure (MAP)
average driving force of blood to the tissues; approximated by taking diastolic pressure and adding 1/3 of pulse pressure
median cubital vein
superficial vessel located in the antecubital region that links the cephalic vein to the basilic vein in the form of a v; a frequent site for a blood draw
median sacral artery
continuation of the aorta into the sacrum
metarteriole
short vessel arising from a terminal arteriole that branches to supply a capillary bed
middle cerebral artery
another branch of the internal carotid artery; supplies blood to the temporal and parietal lobes of the cerebrum
muscular artery
(also, distributing artery) artery with abundant smooth muscle in the tunica media that branches to distribute blood to the arteriole network
myogenic response
constriction or dilation in the walls of arterioles in response to pressures related to blood flow; reduces high blood flow or increases low blood flow to help maintain consistent flow to the capillary network
nervi vasorum
small nerve fibers found in arteries and veins that trigger contraction of the smooth muscle in their walls
net filtration pressure (NFP)
force driving fluid out of the capillary and into the tissue spaces; equal to the difference of the capillary hydrostatic pressure and the blood colloidal osmotic pressure
ophthalmic artery
branch of the internal carotid artery; supplies blood to the eyes
palmar venous arches
drain the hand and digits, and feed into the radial and ulnar veins
parietal branches
(also, somatic branches) group of arterial branches of the thoracic aorta; includes those that supply blood to the thoracic cavity, vertebral column, and the superior surface of the diaphragm
perfusion
distribution of blood into the capillaries so the tissues can be supplied
petrosal sinus
enlarged vein that receives blood from the cavernous sinus and flows into the internal
jugular vein
phrenic vein
drains the diaphragm; the right phrenic vein flows into the inferior vena cava and the left phrenic vein leads to the left renal vein
plantar arch
formed from the anastomosis of the dorsalis pedis artery and medial and plantar arteries; branches supply the distal portions of the foot and digits
plantar veins
drain the foot and lead to the plantar venous arch
popliteal artery
continuation of the femoral artery posterior to the knee; branches into the anterior and posterior tibial arteries
popliteal vein
continuation of the femoral vein behind the knee; drains the region behind the knee and forms from the fusion of the fibular and anterior and posterior tibial veins
posterior tibial artery
branch from the popliteal artery that gives rise to the fibular or peroneal artery; supplies blood to the posterior tibial region
posterior tibial vein
forms from the dorsal venous arch; drains the area near the posterior surface of the tibia and leads to the popliteal vein
precapillary sphincters
circular rings of smooth muscle that surround the entrance to a capillary and regulate blood flow into that capillary
pulmonary circuit
system of blood vessels that provide gas exchange via a network of arteries, veins, and capillaries that run from the heart, through the body, and back to the lungs
pulmonary trunk
single large vessel exiting the right ventricle that divides to form the right and left pulmonary arteries
pulmonary veins
two sets of paired vessels, one pair on each side, that are formed from the small venules leading away from the pulmonary capillaries that flow into the left atrium
pulse
alternating expansion and recoil of an artery as blood moves through the vessel; an indicator of heart rate
pulse pressure
difference between the systolic and diastolic pressures
radial artery
formed at the bifurcation of the brachial artery; parallels the radius; gives off smaller branches until it reaches the carpal region where it fuses with the ulnar artery to form the superficial and deep palmar arches; supplies blood to the lower arm and carpal region
reabsorption
in the cardiovascular system, the movement of material from the interstitial fluid into the capillaries
renal artery
branch of the abdominal aorta; supplies each kidney
renal vein
largest vein entering the inferior vena cava; drains the kidneys and leads to the inferior vena cava
resistance
any condition or parameter that slows or counteracts the flow of blood
respiratory pump
increase in the volume of the thorax during inhalation that decreases air pressure, enabling venous blood to flow into the thoracic region, then exhalation increases pressure, moving blood into the atria
sigmoid sinuses
enlarged veins that receive blood from the transverse sinuses; flow through the jugular foramen and into the internal jugular vein
skeletal muscle pump
effect on increasing blood pressure within veins by compression of the vessel caused by the contraction of nearby skeletal muscle
small saphenous vein
located on the lateral surface of the leg; drains blood from the superficial regions of the lower leg and foot, and leads to the popliteal vein
sphygmomanometer
blood pressure cuff attached to a device that measures blood pressure
splenic artery
branch of the celiac trunk; supplies blood to the spleen
subclavian artery
right subclavian arises from the brachiocephalic artery/trunk, whereas the left subclavian artery arises from the aortic arch; gives rise to the internal thoracic, vertebral, and thyrocervical arteries; supplies blood to the arms, chest, shoulders, back, and central nervous system
subclavian vein
located deep in the thoracic cavity; becomes the axillary vein as it enters the axillary region; drains the axillary and smaller local veins near the scapular region; leads to the brachiocephalic vein
superior mesenteric artery
branch of the abdominal aorta; supplies blood to the small intestine (duodenum, jejunum, and ileum), the pancreas, and a majority of the large intestine
brum and leads to the inferior jugular vein and the vertebral vein
superior vena cava
large systemic vein; drains blood from most areas superior to the diaphragm; empties into the right atrium
systolic pressure
larger number recorded when measuring arterial blood pressure; represents the maximum value following ventricular contraction
thoracic aorta
portion of the descending aorta superior to the aortic hiatus
thoroughfare channel
continuation of the metarteriole that enables blood to bypass a capillary bed and flow directly into a venule, creating a vascular shunt
trunk
large vessel that gives rise to smaller vessels
tunica externa
(also, tunica adventitia) outermost layer or tunic of a vessel (except capillaries)
tunica intima
(also, tunica interna) innermost lining or tunic of a vessel
tunica media
middle layer or tunic of a vessel (except capillaries)
ulnar vein
parallels the ulna and ulnar artery; arises from the palmar venous arches and leads to the brachial vein
vasa vasorum
small blood vessels located within the walls or tunics of larger vessels that supply nourishment to and remove wastes from the cells of the vessels
vascular tone
contractile state of smooth muscle in a blood vessel
vasoconstriction
constriction of the smooth muscle of a blood vessel, resulting in a decreased vascular diameter
vasodilation
relaxation of the smooth muscle in the wall of a blood vessel, resulting in an increased vascular diameter
vasomotion
irregular, pulsating flow of blood through capillaries and related structures
vein
blood vessel that conducts blood toward the heart
venous reserve
volume of blood contained within systemic veins in the integument, bone marrow, and liver that can be returned to the heart for circulation, if needed
venule
small vessel leading from the capillaries to veins
vertebral artery
arises from the subclavian artery and passes through the vertebral foramen through the foramen magnum to the brain; joins with the internal carotid artery to form the arterial circle; supplies blood to the brain and spinal cord
vertebral vein
arises from the base of the brain and the cervical region of the spinal cord; passes through the intervertebral foramina in the cervical vertebrae; drains smaller veins from the cranium, spinal cord, and vertebrae, and leads to the brachiocephalic vein; counterpart of the vertebral artery
Media Attributions
- olelo_noeau
- Formation of New Blood Vessels © Patrycja Kowalska, Foundation of Research and Science Development, Poland is licensed under a CC BY (Attribution) license
- Aʻa Lewalewa © Hawai'i Volcanoes National Park is licensed under a Public Domain license
- Capillaries © National Cancer Institute, National Institutes of Health is licensed under a Public Domain license
- Blood Vessels © Kelvinsong adapted by Begoon is licensed under a CC BY-SA (Attribution ShareAlike) license
- Types of Arteries and Arterioles © OpenStax is licensed under a CC BY (Attribution) license
- Atherosclerosis © OpenStax adapted by LynleyShimat Lys - formatted size to 1mb is licensed under a CC BY (Attribution) license
- RBCs stacking in a capillary © National Heart, Lung, and Blood Institute is licensed under a Public Domain license
- Normal breast histology – Simple squamous epithelium with basement membrane © Mikael Häggström, M.D. is licensed under a CC BY (Attribution) license
- Types of Capillaries © OpenStax is licensed under a CC BY (Attribution) license
- Capillary Bed © OpenStax is licensed under a CC BY (Attribution) license
- Comparison of Veins and Venules © OpenStax is licensed under a CC BY (Attribution) license
- Graphical View of Distribution of Blood Flow © Julie Jenks is licensed under a CC BY (Attribution) license
- Varicose Veins – Leg © Thomas Kriese is licensed under a CC BY (Attribution) license
- Varicose Veins – Inside © Aries Vitality Textiles, a.s. is licensed under a CC BY-SA (Attribution ShareAlike) license
- Varicose Veins – Echogram © BruceBlaus is licensed under a CC BY-SA (Attribution ShareAlike) license
- Illustration of the 3 types of anastomoses © Donato Gerardo Terrone, Luigi Lepanto, Jean-Sébastien Billiard, Damien Olivié, Jessica Murphy-Lavallée, Franck Vandenbroucke & An Tang is licensed under a CC BY-SA (Attribution ShareAlike) license
- The different types of blood vessels © David Nascari and Alan Sved is licensed under a CC BY-SA (Attribution ShareAlike) license
- Angiogenic switch © Mjeltsch is licensed under a CC BY-SA (Attribution ShareAlike) license
- Systemic Blood Pressure © OpenStax is licensed under a CC BY (Attribution) license
- Common pulse points © OpenStax is licensed under a CC BY (Attribution) license
- Stethoscope © Michael is licensed under a CC BY-NC (Attribution NonCommercial) license
- Sphygmometer © Dennis Amith is licensed under a CC BY-NC (Attribution NonCommercial) license
- Akaka Falls © Todd Petit is licensed under a CC BY-NC-SA (Attribution NonCommercial ShareAlike) license
- Water trickling from a drain pipe © andrew is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- Manowaiopuna (“Jurassic”) Falls © Julian Fong is licensed under a CC BY-SA (Attribution ShareAlike) license
- Bowl of poi © Bshams is licensed under a Public Domain license
- Kuʻi Poi (pounding poi) © University of Hawaiʻi - West Oʻahu is licensed under a CC BY-ND (Attribution NoDerivatives) license
- Relationships among Vessels in the Systemic Circuit © OpenStax is licensed under a CC BY (Attribution) license
- Skeletal Muscle Pump © OpenStax is licensed under a CC BY (Attribution) license
- Cardiovascular distribution of blood: Veins and Arteries © Cmglee is licensed under a CC BY-SA (Attribution ShareAlike) license
- Cardiovascular distribution of blood: Table © OpenStax is licensed under a CC BY (Attribution) license
- Hydrostatic and Osmotic Pressure © SGUL lymres is licensed under a CC BY-SA (Attribution ShareAlike) license
- Net filtration pressure along a capillary (Capillary Exchange) © OpenStax is licensed under a CC BY (Attribution) license
- Lymphatic Capillaries © OpenStax is licensed under a CC BY (Attribution) license
- Anatomy of the Lymphatic System © Openstax is licensed under a CC BY (Attribution) license
- Major Trunks and Ducts of the Lymphatic System © OpenStax is licensed under a CC BY (Attribution) license
- Baroreceptor Reflexes © OpenStax is licensed under a CC BY (Attribution) license
- Regulation of Vasodilators: Normal blood vessel (L) Vs. Vasodilation (R) © www.scientificanimations.com is licensed under a CC BY-SA (Attribution ShareAlike) license
- Regulation of Vasodilators: Vasoconstriction © http://www.scientificanimations.com is licensed under a CC BY-SA (Attribution ShareAlike) license
- Myogenic Regulation © Eok-Cheon Kim, Soo-Kyoung Choi, Mihwa Lim, Soo-In Yeon, Young-Ho Lee adapted by LynleyShimat Lys - formatted size to 1mb is licensed under a CC BY (Attribution) license
- Cardiovascular Circulation © OpenStax is licensed under a CC BY (Attribution) license
- Aorta © OpenStax is licensed under a CC BY (Attribution) license
- Arteries and Veins © OpenStax is licensed under a CC BY (Attribution) license
- Systemic Arteries and Veins: Systemic Arteries © OpenStax is licensed under a CC BY (Attribution) license
- Systemic Arteries and Veins: Systemic Veins © OpenStax is licensed under a CC BY (Attribution) license
- Interaction of the Circulatory System with Other Systems © OpenStax adapted by LynleyShimat Lys - resized to 1mb is licensed under a CC BY (Attribution) license
- Coronary Circulation © OpenStax is licensed under a CC BY (Attribution) license
- Internal Structures of the Heart © OpenStax is licensed under a CC BY (Attribution) license
- Arteries Supplying the Head and Neck © OpenStax is licensed under a CC BY (Attribution) license
- Arteries Serving the Brain © OpenStax is licensed under a CC BY (Attribution) license
- Circle of Willis © Openstax is licensed under a CC BY (Attribution) license
- Veins of the Head and Neck © OpenStax is licensed under a CC BY (Attribution) license
- Dural Sinuses and Veins © Openstax is licensed under a CC BY (Attribution) license
- Arteries of the Thoracic and Abdominal Regions © OpenStax is licensed under a CC BY (Attribution) license
- Veins of the Thoracic and Abdominal Regions © OpenStax is licensed under a CC BY (Attribution) license
- Pulmonary Circuit © OpenStax is licensed under a CC BY (Attribution) license
- Esophageal Region: Esophagus © Henry Vandyke Carter, Henry Grey, Warren H. Lewis is licensed under a Public Domain license
- Esophageal Region: Relations of the aorta, trachea, esophagus © Derivative by Mikael Häggström of original by ZooFari. is licensed under a CC BY-SA (Attribution ShareAlike) license
- Esophageal Region: Thoracic Aorta Image © Tiedemann, Friedrich, 1781-1861 is licensed under a Public Domain license
- Esophageal Region: Thoracic Aorta Labels © Tiedemann, Friedrich, 1781-1861 is licensed under a Public Domain license
- Muscles of the Diaphragm © OpenStax is licensed under a CC BY (Attribution) license
- Diaphragm © Tiedemann, Friedrich, 1781-1861 is licensed under a Public Domain license
- Diaphragm Labels 1 © Tiedemann, Friedrich, 1781-1861 is licensed under a Public Domain license
- Diaphragm Labels 2 © Tiedemann, Friedrich, 1781-1861 is licensed under a Public Domain license
- The Celiac Trunk. Pancreas Posterior © Tim Tieu is licensed under a Public Domain license
- The Celiac Trunk. Arterial Blood Supply © Mikael Häggström. is licensed under a Public Domain license
- The Celiac Trunk. Trunk and branches © Henry VanDyke Carter, from Gray's Anatomy by Henry Gray adapted by Dennis M DePace, PhD is licensed under a CC BY-SA (Attribution ShareAlike) license
- Superior and Inferior Mesenteric Arteries. Layers of the Alimentary Canal © OpenStax is licensed under a CC BY (Attribution) license
- Superior and Inferior Mesenteric Arteries. Superior mesenteric artery © Henry Vandyke Carter, from Grey's Anatomy is licensed under a Public Domain license
- Superior and Inferior Mesenteric Arteries. Inferior mesenteric artery © Henry Vandyke Carter, from Grey's Anatomy is licensed under a Public Domain license
- Hepatic Portal System © OpenStax is licensed under a CC BY (Attribution) license
- Hepatic sinusoids. Adult Liver © Zorn, A.M. is licensed under a CC BY (Attribution) license
- Hepatic sinusoids. Liver lobule © Originally by Frevert U, Engelmann S, Zougbédé S, Stange J, Ng B, et al. Converted to SVG by Viacheslav Vtyurin who was hired to do so by User:Eug is licensed under a CC BY (Attribution) license
- Illustration of the Posterior abdominal organs. Posterior Organs © Nanoxyde is licensed under a CC BY-SA (Attribution ShareAlike) license
- Pancreas © OpenStax is licensed under a CC BY (Attribution) license
- Pelvis and perineum vessels © Cunningham, D. J. (Daniel John), 1850-1909; Robinson, Arthur, b. 1862, ed is licensed under a Public Domain license
- Major Arteries Serving the Thorax and Upper Limb © OpenStax is licensed under a CC BY (Attribution) license
- Veins of the Upper Limb © OpenStax is licensed under a CC BY (Attribution) license
- Major Arteries Serving the Lower Limb © OpenStax is licensed under a CC BY (Attribution) license
- Major Veins Serving the Lower Limbs © OpenStax is licensed under a CC BY (Attribution) license
- Honu_‘Iwalani Clayton_CCBY_2022 10 30 © ‘Iwalani Clayton is licensed under a CC BY (Attribution) license
- divider_maile
smallest of blood vessels where physical exchange occurs between the blood and tissue cells surrounded by interstitial fluid
blood vessel that conducts blood toward the heart
(also, tunica interna) innermost lining or tunic of a vessel
middle layer or tunic of a vessel (except capillaries)
constriction of the smooth muscle of a blood vessel, resulting in a decreased vascular diameter
interior of a tubular structure such as a blood vessel or a portion of the alimentary canal through which blood, chyme, or other substances travel
force exerted by the blood against the wall of a vessel or heart chamber; can be described with the more generic term hydrostatic pressure
Widening of blood vessels.
(also, tunica adventitia) outermost layer or tunic of a vessel (except capillaries)
small blood vessels located within the walls or tunics of larger vessels that supply nourishment to and remove wastes from the cells of the vessels
blood vessel that conducts blood away from the heart; may be a conducting or distributing vessel
distribution of blood into the capillaries so the tissues can be supplied
movement of blood through a vessel, tissue, or organ that is usually expressed in terms of volume per unit of time
largest artery in the body, originating from the left ventricle and descending to the abdominal region where it bifurcates into the common iliac arteries at the level of the fourth lumbar vertebra; arteries originating from the aorta distribute blood to virtually all tissues of the body
large arterial vessel that carries blood ejected from the right ventricle; divides into the left and right pulmonary arteries
(also, distributing artery) artery with abundant smooth muscle in the tunica media that branches to distribute blood to the arteriole network
(also, resistance vessel) very small artery that leads to a capillary
the property of electricity whereby the current is impeded in some way
(also, conducting artery) artery with abundant elastic fibers located closer to the heart, which maintains the pressure gradient and conducts blood to smaller branches
small vessel leading from the capillaries to veins
in the cardiovascular system, the movement of material from a capillary into the interstitial fluid, moving from an area of higher pressure to lower pressure
network of 10–100 capillaries connecting arterioles to venules
short vessel arising from a terminal arteriole that branches to supply a capillary bed
continuation of the metarteriole that enables blood to bypass a capillary bed and flow directly into a venule, creating a vascular shunt
circular rings of smooth muscle that surround the entrance to a capillary and regulate blood flow into that capillary
irregular, pulsating flow of blood through capillaries and related structures
short vessel connecting an arteriole directly to a venule and bypassing the capillary beds
superficial vessel in the upper arm; leads to the axillary vein
located deep in the thoracic cavity; becomes the axillary vein as it enters the axillary region; drains the axillary and smaller local veins near the scapular region; leads to the brachiocephalic vein
largest vein entering the inferior vena cava; drains the kidneys and leads to the inferior vena cava
formation of blood capillary networks
alternating expansion and recoil of an artery as blood moves through the vessel; an indicator of heart rate
blood pressure cuff attached to a device that measures blood pressure
continuation of the axillary artery in the brachium; supplies blood to much of the brachial region; gives off several smaller branches that provide blood to the posterior surface of the arm in the region of the elbow; bifurcates into the radial and ulnar arteries at the coronoid fossa
larger number recorded when measuring arterial blood pressure; represents the maximum value following ventricular contraction
lower number recorded when measuring arterial blood pressure; represents the minimal value corresponding to the pressure that remains during ventricular relaxation
difference between the systolic and diastolic pressures
average driving force of blood to the tissues; approximated by taking diastolic pressure and adding 1/3 of pulse pressure
a reduction in blood flow that results in hypoxia (insufficient delivery of oxygen to the cells and tissues of the body)
lack of oxygen supply to the tissues
formed at the bifurcation of the brachial artery; parallels the radius; gives off smaller branches until it reaches the carpal region where it fuses with the ulnar artery to form the superficial and deep palmar arches; supplies blood to the lower arm and carpal region
right common carotid artery arises from the brachiocephalic artery, and the left common carotid arises from the aortic arch; gives rise to the external and internal carotid arteries; supplies the respective sides of the head and neck
noises created by turbulent blood flow through the vessels
abnormally low levels of fluid and blood within the body
type of circulatory shock caused by excessive loss of blood volume due to hemorrhage or possibly dehydration
also simply called shock; a life-threatening medical condition in which the circulatory system is unable to supply enough blood flow to provide adequate oxygen and other nutrients to the tissues to maintain cellular metabolism
abnormally high levels of fluid and blood within the body
chronic and persistent blood pressure measurements of 140/90 mm Hg or above
contractile state of smooth muscle in a blood vessel
degree to which a blood vessel can stretch as opposed to being rigid
effect on increasing blood pressure within veins by compression of the vessel caused by the contraction of nearby skeletal muscle
large vessel that gives rise to smaller vessels
increase in the volume of the thorax during inhalation that decreases air pressure, enabling venous blood to flow into the thoracic region, then exhalation increases pressure, moving blood into the atria
ability of a vein to distend and store blood
volume of blood contained within systemic veins in the integument, bone marrow, and liver that can be returned to the heart for circulation, if needed
in the cardiovascular system, the movement of material from the interstitial fluid into the capillaries
force blood exerts against the walls of a blood vessel or heart chamber
force blood exerts against a capillary
force exerted by the fluid in the tissue spaces
pressure exerted by colloids suspended in blood within a vessel; a primary determinant is the presence of plasma proteins
pressure exerted by the colloids within the interstitial fluid
force driving fluid out of the capillary and into the tissue spaces; equal to the difference of the capillary hydrostatic pressure and the blood colloidal osmotic pressure
small nerve fibers found in arteries and veins that trigger contraction of the smooth muscle in their walls
small pockets in the ascending aorta near the aortic valve that are the locations of the baroreceptors (stretch receptors) and chemoreceptors that trigger a reflex that aids in the regulation of vascular homeostasis
initial portion of the aorta, rising from the left ventricle for a distance of approximately 5 cm
small pockets near the base of the internal carotid arteries that are the locations of the baroreceptors and chemoreceptors that trigger a reflex that aids in the regulation of vascular homeostasis
(also, called Bainbridge reflex) autonomic reflex that responds to stretch receptors in the atria that send impulses to the cardioaccelerator area to increase HR when venous flow into the atria increases
constriction or dilation in the walls of arterioles in response to pressures related to blood flow; reduces high blood flow or increases low blood flow to help maintain consistent flow to the capillary network
blood flow to and from the lungs
veins that carry highly oxygenated blood into the left atrium, which pumps the blood into the left ventricle, which in turn pumps oxygenated blood into the aorta and to the many branches of the systemic circuit
descends toward the inferior portions of the body and ends at the level of the intervertebral disk between the fourth and fifth thoracic vertebrae
right subclavian arises from the brachiocephalic artery/trunk, whereas the left subclavian artery arises from the aortic arch; gives rise to the internal thoracic, vertebral, and thyrocervical arteries; supplies blood to the arms, chest, shoulders, back, and central nervous system
portion of the aorta that continues downward past the end of the aortic arch; subdivided into the thoracic aorta and the abdominal aorta
portion of the descending aorta superior to the aortic hiatus
portion of the aorta inferior to the aortic hiatus and superior to the common iliac
arteries
large systemic vein that returns blood to the heart from the inferior portion of the body
large systemic vein that returns blood to the heart from the superior portion of the body
one of a pair of veins that form from a fusion of the external and internal jugular veins and the subclavian vein; subclavian, external and internal jugulars, vertebral, and internal thoracic veins lead to it; drains the upper thoracic region and flows into the superior vena cava
arises from the subclavian artery and passes through the vertebral foramen through the foramen magnum to the brain; joins with the internal carotid artery to form the arterial circle; supplies blood to the brain and spinal cord
arises from the common carotid artery; supplies blood to numerous structures within the face, lower jaw, neck, esophagus, and larynx
another branch of the internal carotid artery; supplies blood to the temporal and parietal lobes of the cerebrum
branch of the internal carotid artery; supplies blood to the eyes
blood vessel from the merged vertebral arteries that runs along the dorsal surface of the brain stem
unique anatomical arrangement of blood vessels around the base of the brain that maintains perfusion of blood into the brain even if one component of the structure is blocked or narrowed
branch from the common carotid artery that enters the cranium and supplies blood to the brain
continuation of the subclavian artery as it penetrates the body wall and enters the axillary region; supplies blood to the region near the head of the humerus (humeral circumflex arteries); the majority of the vessel continues into the brachium and becomes the brachial artery
(also, circle of Willis) anastomosis located at the base of the brain that ensures continual blood supply; formed from branches of the internal carotid and vertebral arteries; supplies blood to the brain
one of a pair of major veins located in the superficial neck region that drains blood from the more superficial portions of the head, scalp, and cranial regions, and leads to the subclavian vein
arises from the base of the brain and the cervical region of the spinal cord; passes through the intervertebral foramina in the cervical vertebrae; drains smaller veins from the cranium, spinal cord, and vertebrae, and leads to the brachiocephalic vein; counterpart of the vertebral artery
one of a pair of major veins located in the neck region that passes through the jugular foramen and canal, flows parallel to the common carotid artery that is more or less its counterpart; primarily drains blood from the brain, receives the superficial facial vein, and empties into the subclavian vein
receives most of the smaller vessels from the inferior cerebral veins and leads to the straight sinus
enlarged vein that receives blood from the cavernous sinus and flows into the internal
jugular vein
dural sinuses that drain directly into the jugular veins
branches of the abdominal aorta; supply blood to the lumbar region, the abdominal wall, and spinal cord
continuation of the aorta into the sacrum
(also, mammary artery) arises from the subclavian artery; supplies blood to the thymus, pericardium of the heart, and the anterior chest wall
(also, somatic branches) group of arterial branches of the thoracic aorta; includes those that supply blood to the thoracic cavity, vertebral column, and the superior surface of the diaphragm
(also, internal mammary vein) drains the anterior surface of the chest wall and leads to the brachiocephalic vein
formed when the femoral vein passes into the body cavity; drains the legs and leads to the common iliac vein
drains the muscles of the thoracic wall and leads to the azygos vein
smaller vein complementary to the azygos vein; drains the esophageal veins from the esophagus and the left intercostal veins, and leads to the brachiocephalic vein via the superior intercostal vein
originates in the lumbar region and passes through the diaphragm into the thoracic cavity on the right side of the vertebral column; drains blood from the intercostal veins, esophageal veins, bronchial veins, and other veins draining the mediastinal region; leads to the superior vena cava
drains the systemic circulation from the lungs and leads to the azygos vein
branch of the celiac trunk; supplies blood to the stomach
drains the inferior portions of the esophagus and leads to the azygos vein
drains the diaphragm; the right phrenic vein flows into the inferior vena cava and the left phrenic vein leads to the left renal vein
(also, celiac artery) major branch of the abdominal aorta; gives rise to the left gastric artery, the splenic artery, and the common hepatic artery that forms the hepatic artery to the liver, the right gastric artery to the stomach, and the cystic artery to the gallbladder
branch of the celiac trunk; supplies blood to the spleen
branch of the celiac trunk that forms the hepatic artery, the right gastric artery, and the cystic artery
branch of the common hepatic artery; supplies systemic blood to the liver
branch of the abdominal aorta; supplies blood to the small intestine (duodenum, jejunum, and ileum), the pancreas, and a majority of the large intestine
branch of the abdominal aorta; supplies blood to the distal segment of the large intestine and rectum
specialized circulatory pathway that carries blood from digestive organs to the liver for processing before being sent to the systemic circulation
drains systemic blood from the liver and flows into the inferior vena cava
branch of the abdominal aorta; supplies each kidney
branch of the abdominal aorta; supplies blood to the gonads or reproductive organs; also described as ovarian arteries or testicular arteries, depending upon the sex of the individual
branch from the common iliac arteries; supplies blood to the urinary bladder, walls of the pelvis, external genitalia, and the medial portion of the femoral region; in females, also provide blood to the uterus and vagina
drains the pelvic organs and integument; formed from several smaller veins in the region; leads to the common iliac vein
one of a pair of veins that flows into the inferior vena cava at the level of L5; the left common iliac vein drains the sacral region; divides into external and internal iliac veins near the inferior portion of the sacroiliac joint
formed from the superficial and deep palmar arches; supply blood to the digits
superficial vein of the arm that arises from the palmar venous arches, intersects with the median cubital vein, parallels the ulnar vein, and continues into the upper arm; along with the brachial vein, it leads to the axillary vein
major vein in the axillary region; drains the upper limb and becomes the subclavian vein
superficial vessel located in the antecubital region that links the cephalic vein to the basilic vein in the form of a v; a frequent site for a blood draw
drain the digits and feed into the palmar arches of the hand and dorsal venous arch of the foot
drain the hand and digits, and feed into the radial and ulnar veins
parallels the ulna and ulnar artery; arises from the palmar venous arches and leads to the brachial vein
deeper vein of the arm that forms from the radial and ulnar veins in the lower arm; leads to the axillary vein
branch of the common iliac artery that leaves the body cavity and becomes a femoral artery; supplies blood to the lower limbs
branch of the aorta that leads to the internal and external iliac arteries
continuation of the external iliac artery after it passes through the body cavity; divides into several smaller branches, the lateral deep femoral artery, and the genicular artery; becomes the popliteal artery as it passes posterior to the knee
branch of the femoral artery; gives rise to the lateral circumflex arteries
continuation of the femoral artery posterior to the knee; branches into the anterior and posterior tibial arteries
branches from the popliteal artery; supplies blood to the anterior tibial region; becomes the dorsalis pedis artery
forms from the anterior tibial artery; branches repeatedly to supply blood to the tarsal and dorsal regions of the foot
branch from the popliteal artery that gives rise to the fibular or peroneal artery; supplies blood to the posterior tibial region
arises from the bifurcation of the posterior tibial arteries; supplies blood to the lateral plantar surfaces of the foot
formed from the anastomosis of the dorsalis pedis artery and medial and plantar arteries; branches supply the distal portions of the foot and digits
drains blood from digital veins and vessels on the superior surface of the foot
located on the lateral surface of the leg; drains blood from the superficial regions of the lower leg and foot, and leads to the popliteal vein
prominent surface vessel located on the medial surface of the leg and thigh; drains the superficial portions of these areas and leads to the femoral vein
drains the upper leg; receives blood from the great saphenous vein, the deep femoral vein, and the femoral circumflex vein; becomes the external iliac vein when it crosses the body wall
continuation of the femoral vein behind the knee; drains the region behind the knee and forms from the fusion of the fibular and anterior and posterior tibial veins
drain the foot and lead to the plantar venous arch
forms from the dorsal venous arch; drains the area near the posterior surface of the tibia and leads to the popliteal vein
drains the muscles and integument near the fibula and leads to the popliteal vein
forms from the dorsal venous arch; drains the area near the tibialis anterior muscle and leads to the popliteal vein

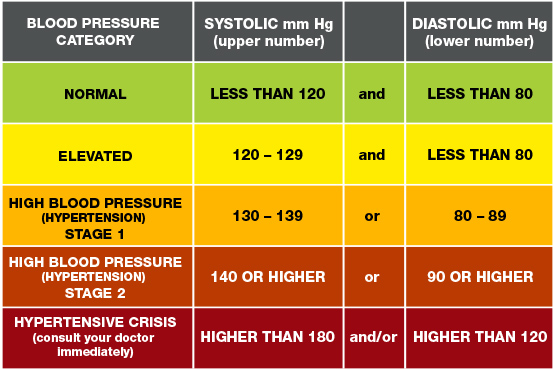{kind=link}
_Falls.jpg){kind=link}
{kind=link}
{kind=link}
_-en.svg){kind=link}
{kind=link}
{kind=link}
{kind=link}
.png){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_(14598327757).jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_(20629111828).jpg){kind=link}